Mathew Gisha V, Shibli Khalil, Korichi Noureddine, Thippeswamy Venkatesh B
Anaesthesia, Hamad Medical Corporation, Doha, QAT.
Cureus. 2021 Aug 5;13(8):e16915. doi: 10.7759/cureus.16915. eCollection 2021 Aug.
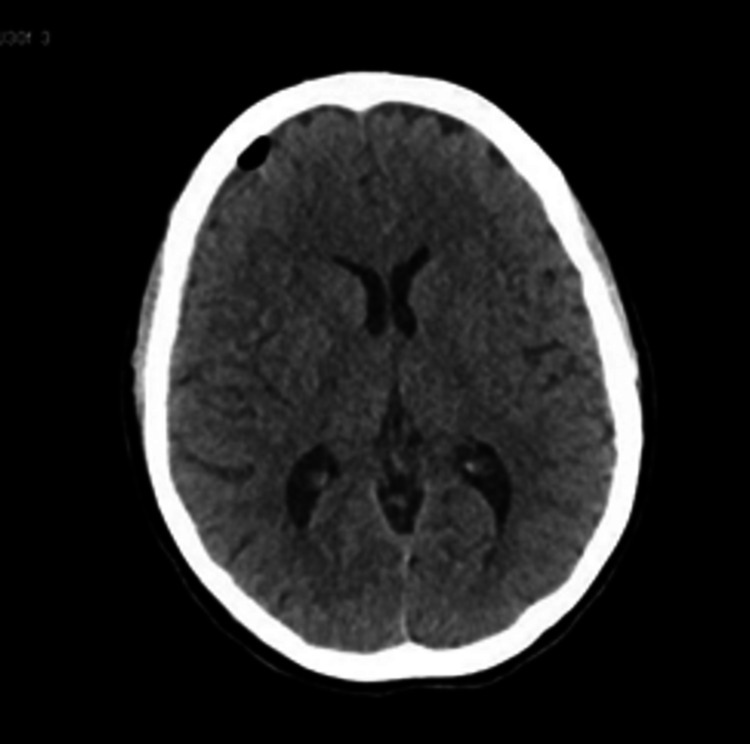
Inadvertent dural puncture with subsequent post-dural puncture headache (PDPH) is the most typical complication of labour epidural analgesia. Subdural hematoma (SDH) is a rare but late neurological complication of this procedure. The intracranial hypotension created by the cerebrospinal fluid (CSF) leakage through the dural defect can lead to the rupture of the bridging veins to produce a subdural hematoma. A change in the character from postural to a non-postural headache is a warning sign of subdural hematoma. We describe a case of post-dural puncture headache followed by the development of cranial SDH in a patient who refused a blood patch and opted for conservative treatment. We conclude that a high index of suspicion must be maintained with a witnessed dural puncture or even without it but having persistent headache, to detect any severe complications like an intracranial subdural hematoma. An epidural blood patch is to be considered when the headache does not subside with conservative management. Early employment of MRI or CT head imaging studies should be considered to exclude, diagnose, or treat any serious complication without unnecessary delay.
分娩硬膜外镇痛最典型的并发症是意外硬膜穿刺及随后的硬膜穿刺后头痛(PDPH)。硬膜下血肿(SDH)是该操作罕见但较迟出现的神经并发症。脑脊液通过硬膜缺损漏出导致的颅内低压可致使桥静脉破裂,进而形成硬膜下血肿。头痛性质从体位性转变为非体位性是硬膜下血肿的警示信号。我们报告一例硬膜穿刺后头痛患者,随后发生了颅内硬膜下血肿,该患者拒绝接受血补丁治疗而选择保守治疗。我们得出结论,对于有硬膜穿刺见证或即使没有见证但存在持续性头痛的情况,必须保持高度怀疑,以发现任何严重并发症,如颅内硬膜下血肿。当头痛经保守治疗不缓解时,应考虑进行硬膜外血补丁治疗。应尽早进行头颅MRI或CT影像学检查,以排除、诊断或治疗任何严重并发症,避免不必要的延误。