Piscoya Alejandro, Ng-Sueng Luis F, Parra Del Riego Angela, Cerna-Viacava Renato, Pasupuleti Vinay, Thota Priyaleela, Roman Yuani M, Hernandez Adrian V
Unidad de Revisiones Sistemáticas y Meta-análisis, Guías de Práctica Clínica y Evaluaciones de Tecnologías Sanitarias (URSIGET), Universidad San Ignacio de Loyola, Lima, Peru.
Hospital Guillermo Kaelin de la Fuente, Lima, Peru.
Arch Med Sci. 2021 Feb 18;17(5):1251-1261. doi: 10.5114/aoms/132492. eCollection 2021.
We systematically reviewed benefits and harms of convalescent plasma (CP) in hospitalized COVID-19 patients.
Randomized controlled trials (RCTs) and observational studies assessing CP effects on hospitalized, adult COVID-19 patients were searched until November 24, 2020. We assessed risk of bias (RoB) using Cochrane RoB 2.0 and ROBINS-I tools. Inverse variance random effect meta-analyses were performed. Quality of evidence was evaluated using GRADE methodology. Primary outcomes were all-cause mortality, clinical improvement, and adverse events.
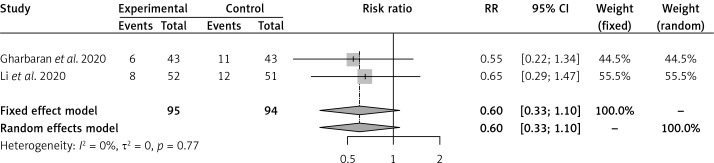
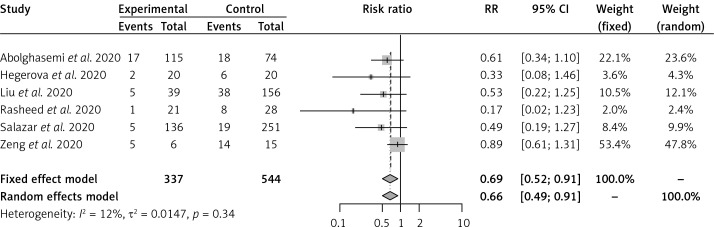
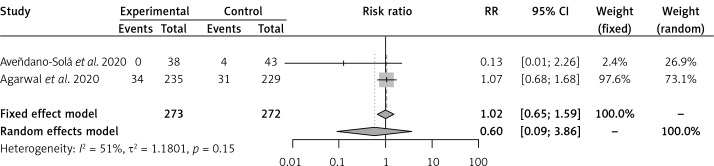
Five RCTs ( = 1067) and 6 cohorts ( = 881) were included. Three and 1 RCTs had some concerns and high RoB, respectively; and there was serious RoB in all cohorts. Convalescent plasma did not reduce all-cause mortality in RCTs of severe (RR = 0.60, 95% CI: 0.33-1.10) or moderate (RR = 0.60, 95% CI: 0.09-3.86) COVID-19 vs. standard of care (SOC); CP reduced all-cause mortality vs. SOC in cohorts (RR = 0.66, 95% CI: 0.49-0.91). Convalescent plasma did not reduce invasive ventilation vs. SOC in moderate disease (RR = 0.85, 95% CI: 0.47-1.55). In comparison to placebo + SOC, CP did not affect all-cause mortality (RR = 0.75, 95% CI: 0.48-1.16) or clinical improvement (HR = 1.07, 95% CI: 0.82-1.40) in severe patients. Adverse and serious adverse events were scarce, similar between CP and controls. Quality of evidence was low or very low for most outcomes.
In comparison to SOC or placebo + SOC, CP did not reduce all-cause mortality in RCTs of hospitalized COVID-19 patients. Convalescent plasma did not have an effect on other clinical or safety outcomes. Until now there is no good quality evidence to recommend CP for hospitalized COVID-19 patients.
我们系统回顾了恢复期血浆(CP)对住院的COVID-19患者的利弊。
检索截至2020年11月24日评估CP对住院成年COVID-19患者影响的随机对照试验(RCT)和观察性研究。我们使用Cochrane RoB 2.0和ROBINS-I工具评估偏倚风险(RoB)。进行了逆方差随机效应荟萃分析。使用GRADE方法评估证据质量。主要结局为全因死亡率、临床改善情况和不良事件。
纳入了5项RCT(n = 1067)和6项队列研究(n = 881)。分别有3项和1项RCT存在一些担忧和高RoB;所有队列研究均存在严重RoB。在重度(RR = 0.60,95%CI:0.33 - 1.10)或中度(RR = 0.60,95%CI:0.09 - 3.86)COVID-19的RCT中,与标准治疗(SOC)相比,恢复期血浆未降低全因死亡率;在队列研究中,与SOC相比,CP降低了全因死亡率(RR = 0.66,95%CI:0.49 - 0.91)。在中度疾病中,与SOC相比,恢复期血浆未降低有创通气率(RR = 0.85,95%CI:0.47 - 1.55)。与安慰剂 + SOC相比,CP对重度患者的全因死亡率(RR = 0.75,95%CI:0.48 - 1.16)或临床改善情况(HR = 1.07,95%CI:0.82 - 1.40)无影响。不良事件和严重不良事件较少,CP组与对照组相似。大多数结局的证据质量为低或极低。
与SOC或安慰剂 + SOC相比,在住院COVID-19患者的RCT中,CP未降低全因死亡率。恢复期血浆对其他临床或安全性结局无影响。目前尚无高质量证据推荐对住院COVID-19患者使用CP。