Department of Family Social Science, University of Minnesota, Minneapolis, MN, USA.
Department of Family Medicine and Community Health, University of Minnesota, Minneapolis, MN, USA.
Adm Policy Ment Health. 2022 Mar;49(2):312-325. doi: 10.1007/s10488-021-01165-z. Epub 2021 Sep 16.
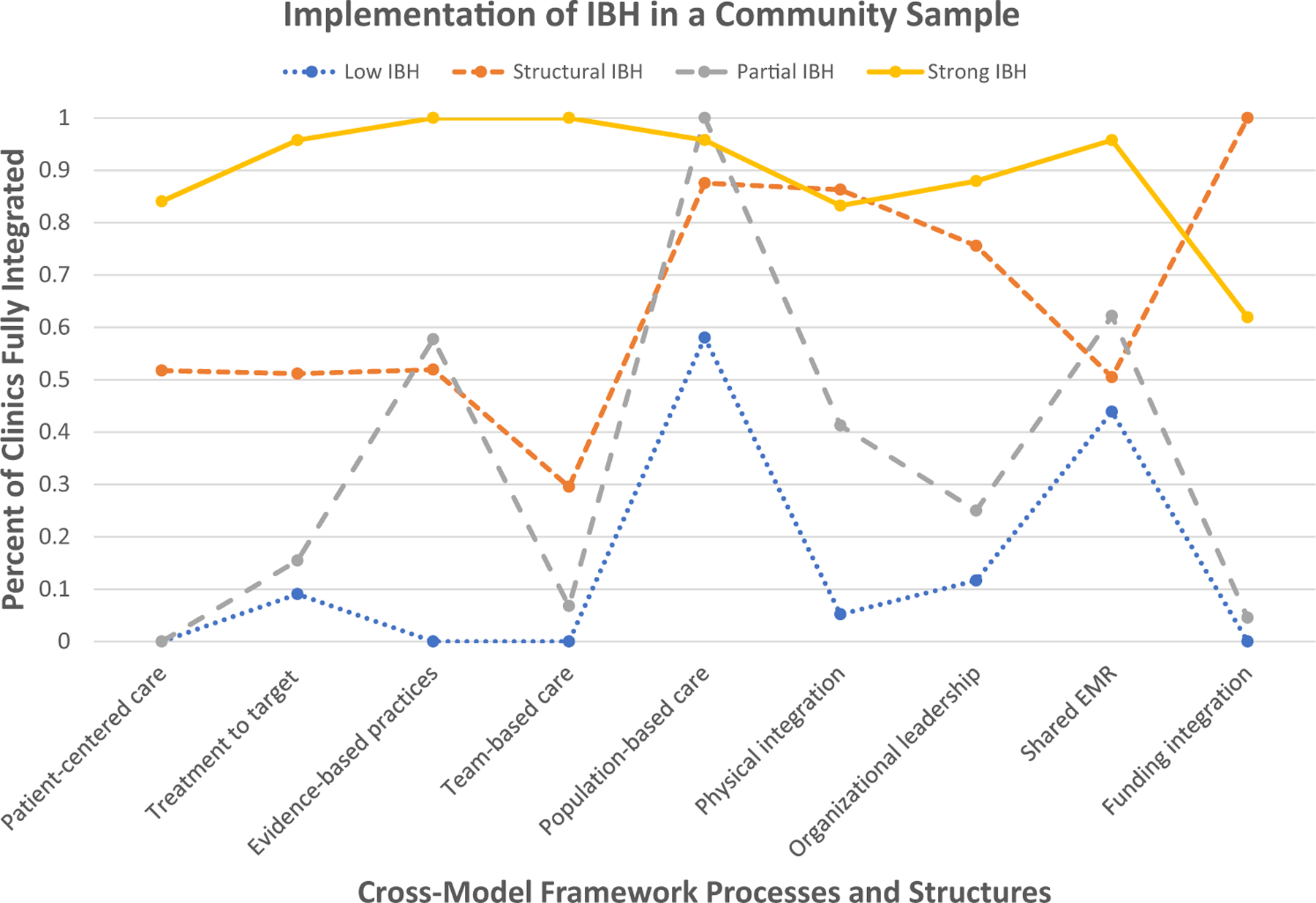
Primary care has increasingly adopted integrated behavioral health (IBH) practices to enhance overall care. The IBH Cross-Model Framework clarifies the core processes and structures of IBH, but little is known about how practices vary in the implementation of these processes and structures. This study aimed to describe clusters of clinics using the IBH Cross-Model Framework for a large sample of primary care clinics, as well as contextual variables associated with differences in implementation. Primary care clinics (N = 102) in Minnesota reported their level of implementation across 18 different components of IBH via the site self-assessment (SSA). The components were mapped to all five principles and four of the nine structures of the IBH Cross-Model Framework. latent class analysis was used to identify unique clusters of IBH components from the SSA across the IBH Cross-Model Framework's processes and structures. Latent classes were then regressed onto context variables. A four-class model was determined to be the best fit: Low IBH (39.6%), Structural IBH (7.9%), Partial IBH (29.4%), and Strong IBH (23.1%). Partial IBH clinics were more urban than the other three classes, lower in SES risk than Structural IBH clinics, and located in smaller organizations than Strong IBH clinics. There were no differences between classes in race/ethnicity of the clinic area or practice size. Four groups of IBH implementation were identified representing unique profiles of integration. These clusters may represent patterns of community-based implementation of IBH that indicate easier and more challenging aspects of IBH implementation.
初级保健越来越多地采用综合行为健康(IBH)实践来增强整体护理。IBH 跨模式框架阐明了 IBH 的核心流程和结构,但对于实践在这些流程和结构的实施中如何存在差异知之甚少。本研究旨在使用 IBH 跨模式框架描述大量初级保健诊所的诊所集群,以及与实施差异相关的背景变量。明尼苏达州的初级保健诊所(N=102)通过现场自我评估(SSA)报告了他们在 IBH 跨模式框架的 18 个不同组成部分中的实施水平。这些组件映射到 IBH 跨模式框架的五个原则和四个结构中的九个结构。使用潜在类别分析从 SSA 中识别 IBH 组件在 IBH 跨模式框架的流程和结构上的独特集群。然后将潜在类别回归到上下文变量。确定四类别模型是最佳拟合:低 IBH(39.6%)、结构 IBH(7.9%)、部分 IBH(29.4%)和强 IBH(23.1%)。部分 IBH 诊所比其他三个类别更城市化,SES 风险低于结构 IBH 诊所,并且位于比强 IBH 诊所更小的组织中。诊所所在地区的种族/族裔或诊所规模在不同类别之间没有差异。确定了四个 IBH 实施组,代表了整合的独特特征。这些集群可能代表了基于社区的 IBH 实施模式,表明了 IBH 实施的更容易和更具挑战性的方面。