Tamale Teaching Hospital, COVID-19 Management Team, Accra, Ghana.
Community Health Department, University of Ghana Medical School, Accra, Ghana.
PLoS One. 2021 Sep 17;16(9):e0257450. doi: 10.1371/journal.pone.0257450. eCollection 2021.
Coronavirus disease-19 (COVID-19), which started in late December, 2019, has spread to affect 216 countries and territories around the world. Globally, the number of cases of SARS-CoV-2 infection has been growing exponentially. There is pressure on countries to flatten the curves and break transmission. Most countries are practicing partial or total lockdown, vaccination, massive education on hygiene, social distancing, isolation of cases, quarantine of exposed and various screening approaches such as temperature and symptom-based screening to break the transmission. Some studies outside Africa have found the screening for fever using non-contact thermometers to lack good sensitivity for detecting SARS-CoV-2 infection. The aim of this study was to determine the usefulness of clinical symptoms in accurately predicting a final diagnosis of COVID-19 disease in the Ghanaian setting.
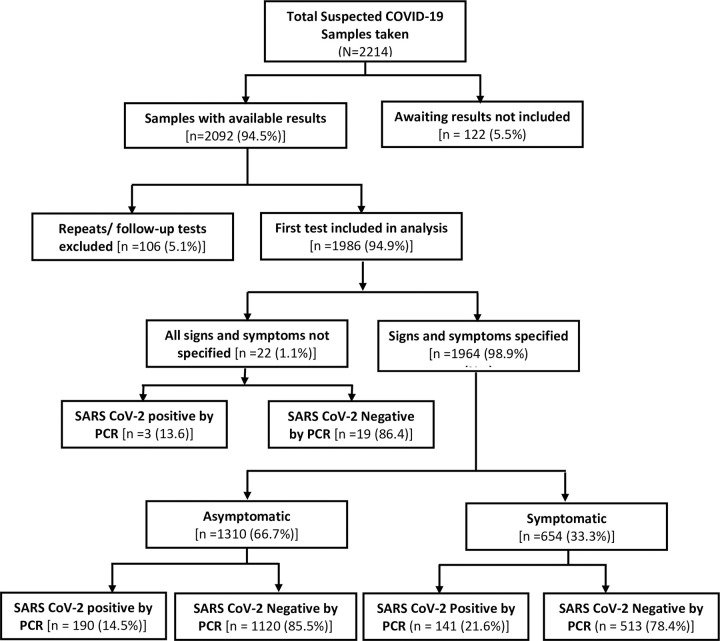
The study analysed screening and test data of COVID-19 suspected, probable and contacts for the months of March to August 2020. A total of 1,986 participants presenting to Tamale Teaching hospital were included in the study. Logistic regression and receiver operator characteristics (ROC) analysis were carried out.
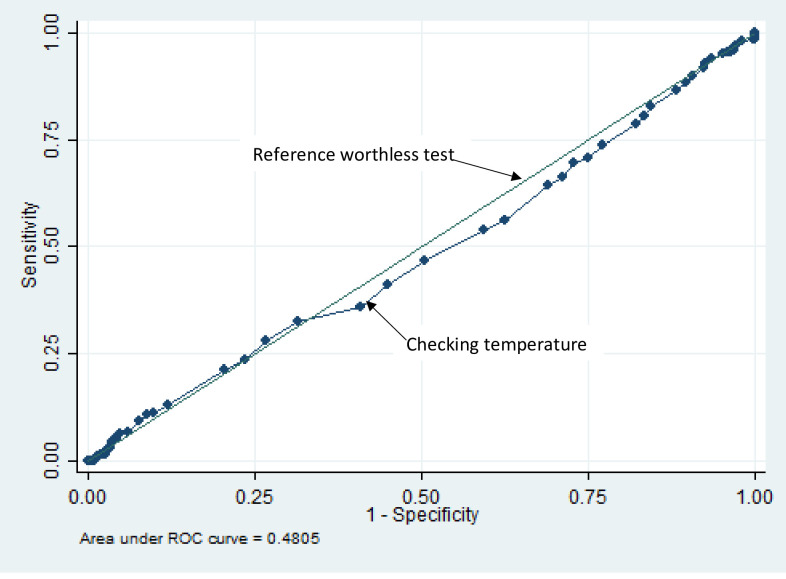
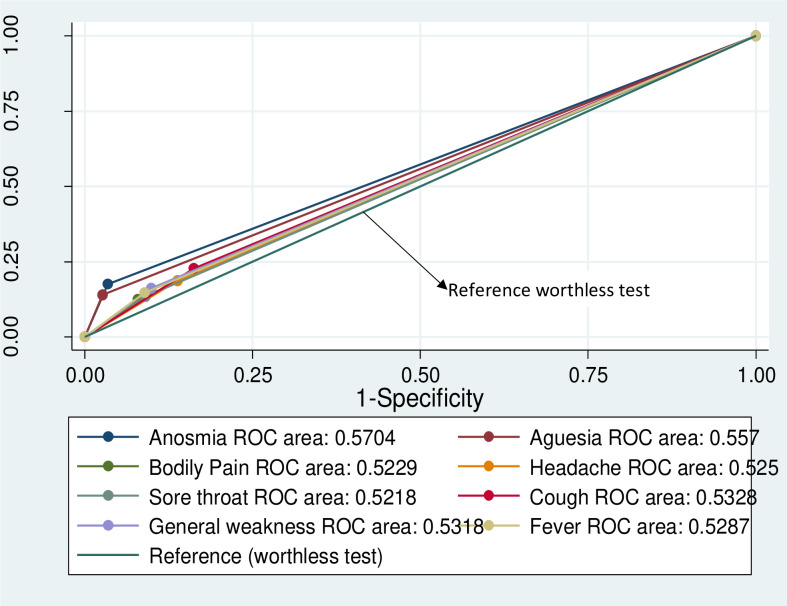
Overall SARS-CoV-2 positivity rate was 16.8%. Those with symptoms had significantly higher positivity rate (21.6%) compared with asymptomatic (17.0%) [chi-squared 15.5, p-value, <0.001]. Patients that were positive for SARS-CoV-2 were 5.9 [3.9-8.8] times more likely to have loss of sense of smell and 5.9 [3.8-9.3] times more likely to having loss of sense of taste. Using history of fever as a screening tool correctly picked up only 14.8% of all true positives of SARS-CoV-2 infection and failed to pick up 86.2% of positive cases. Using cough alone would detect 22.4% and miss 87.6%. Non-contact thermometer used alone, as a screening tool for COVID-19 at a cut-off of 37.8 would only pick 4.8% of positive SARS-CoV-2 infected patients.
The use of fever alone or other symptoms individually [or in combination] as a screening tool for SARS-CoV-2 infection is not worthwhile based on ROC analysis. Use of temperature check as a COVID-19 screening tool to allow people into public space irrespective of the temperature cut-off is of little benefit in diagnosing infected persons. We recommend the use of facemask, hand hygiene, social distancing as effective means of preventing infection.
2019 年 12 月下旬开始的新型冠状病毒病(COVID-19)已蔓延至全球 216 个国家和地区。全球 SARS-CoV-2 感染病例呈指数级增长。各国面临着使曲线变平并阻断传播的压力。大多数国家实行部分或全面封锁、接种疫苗、大规模开展卫生教育、保持社交距离、隔离病例、对暴露者进行检疫以及各种筛查方法,如基于体温和症状的筛查,以阻断传播。一些非非洲地区的研究发现,使用非接触式温度计筛查发热对检测 SARS-CoV-2 感染的敏感性较差。本研究旨在确定在加纳环境中,临床症状在准确预测 COVID-19 疾病的最终诊断方面的有用性。
本研究分析了 2020 年 3 月至 8 月 COVID-19 疑似、可能和接触者的筛查和检测数据。共有 1986 名到塔马利教学医院就诊的患者纳入研究。进行了逻辑回归和接收者操作特征(ROC)分析。
总体 SARS-CoV-2 阳性率为 16.8%。有症状者的阳性率(21.6%)明显高于无症状者(17.0%)[卡方值 15.5,p 值<0.001]。SARS-CoV-2 阳性患者发生嗅觉丧失的可能性高 5.9 倍[3.9-8.8],味觉丧失的可能性高 5.9 倍[3.8-9.3]。将发热史作为筛查工具,仅正确识别了 SARS-CoV-2 感染的所有真阳性病例的 14.8%,而漏诊了 86.2%的阳性病例。仅使用咳嗽,可检出 22.4%,漏诊 87.6%。使用非接触式温度计作为筛查工具,截断值为 37.8°C,仅能检出 4.8%的 SARS-CoV-2 感染阳性患者。
根据 ROC 分析,单独使用发热或其他症状[或组合使用]作为 SARS-CoV-2 感染的筛查工具是不值得的。使用体温检查作为 COVID-19 筛查工具,允许体温高于或低于截断值的人进入公共场所,对诊断感染者几乎没有益处。我们建议使用口罩、手部卫生、保持社交距离作为预防感染的有效手段。