Department of Hepatobiliary and Pancreatic Surgery, National Cancer Center Hospital East, Kashiwa, Japan.
Clinical Research Support Office, National Cancer Center Hospital East, Kashiwa, Japan.
Cancer Med. 2021 Oct;10(20):6998-7011. doi: 10.1002/cam4.4227. Epub 2021 Sep 18.
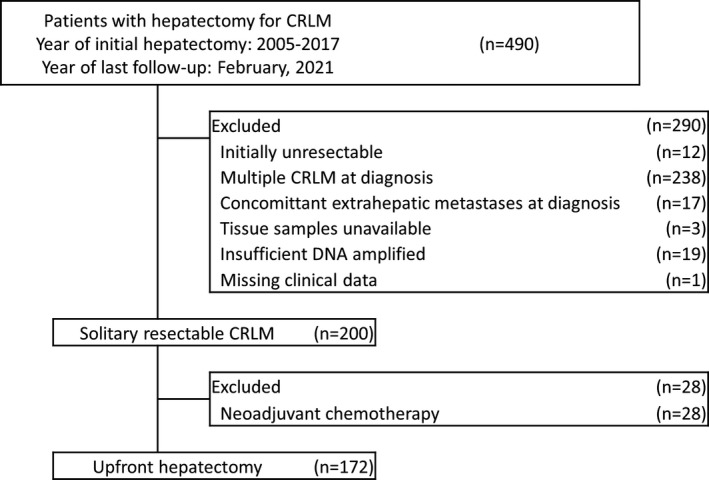
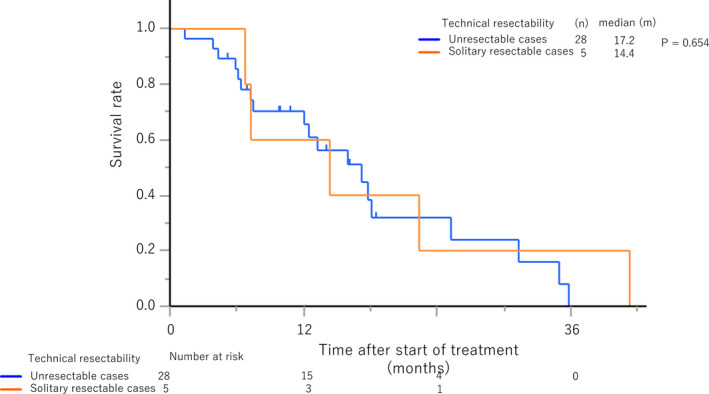
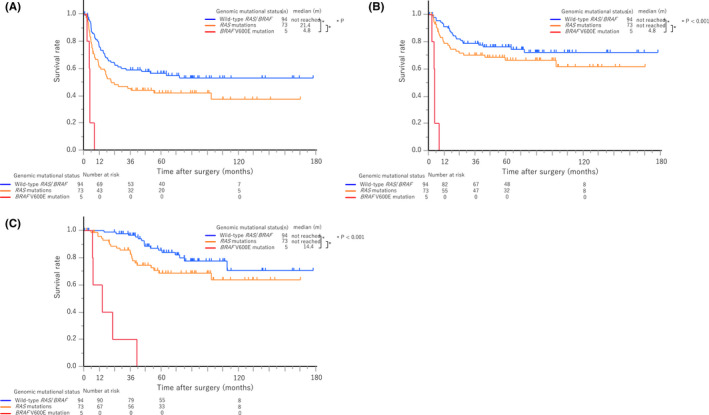
Despite reports on poor survival outcomes after hepatectomy for colorectal liver metastases (CRLM) with BRAF V600E mutation (mBRAF) exist, the role of mBRAF testing for technically resectable cases remains unclear. A single-center retrospective study was performed to investigate the survival outcomes of patients who underwent upfront hepatectomy for solitary resectable CRLM with mBRAF between January 2005 and December 2017 and to compare them with those of unresectable cases with mBRAF. Of 172 patients who underwent initial hepatectomy for solitary resectable CRLM, mBRAF, RAS mutations (mRAS), and wild-type RAS/BRAF (wtRAS/BRAF) were observed in 5 (2.9%), 73 (42.4%), and 93 (54.7%) patients, respectively. With a median follow-up period of 72.8 months, mBRAF was associated with a significantly shorter OS (median, 14.4 months) than wtRAS/BRAF (median, not reached [NR]) (hazard ratio [HR], 27.6; p < 0.001) and mRAS (median, NR) (HR, 9.9; p < 0.001), and mBRAF had the highest HR among all the indicators in the multivariable analysis (HR, 17.0; p < 0.001). The median OS after upfront hepatectomy for CRLM with mBRAF was identical to that of 28 unresectable CRLM with mBRAF that were treated with systemic chemotherapy (median, 17.2 months) (HR, 0.78; p = 0.65). When technically resectable CRLM are complicated with mBRAF, its survival outcome becomes as poor as unresectable cases; therefore, those with mBRAF should be considered as oncologically unresectable. Patients with CRLM should undergo pre-treatment mBRAF testing regardless of technical resectability. Clinical trial registration number: UMIN000034557.
尽管已有报道称结直肠肝转移(CRLM)患者行肝切除术并伴有 BRAF V600E 突变(mBRAF)时预后较差,但 mBRAF 检测在技术上可切除病例中的作用仍不清楚。本研究为单中心回顾性研究,旨在探讨 2005 年 1 月至 2017 年 12 月期间因单发可切除 CRLM 而接受初始肝切除术且伴有 mBRAF 的患者的生存结局,并与伴有 mBRAF 的不可切除病例进行比较。在 172 例接受初始肝切除术治疗单发可切除 CRLM 的患者中,5 例(2.9%)、73 例(42.4%)和 93 例(54.7%)患者分别存在 mBRAF、RAS 突变(mRAS)和野生型 RAS/BRAF(wtRAS/BRAF)。中位随访 72.8 个月后,mBRAF 患者的 OS(中位:14.4 个月)明显短于 wtRAS/BRAF(中位:未达到[NR])(风险比[HR]:27.6;p<0.001)和 mRAS(中位:NR)(HR:9.9;p<0.001),且在多变量分析中,mBRAF 是所有指标中 HR 最高的(HR:17.0;p<0.001)。伴有 mBRAF 的 CRLM 行初始肝切除术的中位 OS 与 28 例接受系统化疗的不可切除伴有 mBRAF 的 CRLM 相同(中位:17.2 个月)(HR:0.78;p=0.65)。当技术上可切除的 CRLM 伴有 mBRAF 时,其生存结局与不可切除病例一样差;因此,伴有 mBRAF 的患者应被视为具有不可切除的肿瘤学特征。无论技术可切除性如何,患有 CRLM 的患者均应进行治疗前 mBRAF 检测。临床试验注册号:UMIN000034557。