Waring Olivia J, Skenteris Nikolaos T, Biessen Erik A L, Donners Marjo M P C
Department of Pathology, Cardiovascular Research Institute Maastricht (CARIM), Maastricht University Medical Center, P. Debyelaan 25, 6229 HX, Maastricht, The Netherlands.
Cardiovascular Medicine Unit, Department of Medicine, Karolinska Institutet, Visionsgatan 4, 171 64, Solna, Sweden.
Cardiovasc Res. 2022 Oct 21;118(13):2768-2777. doi: 10.1093/cvr/cvab301.
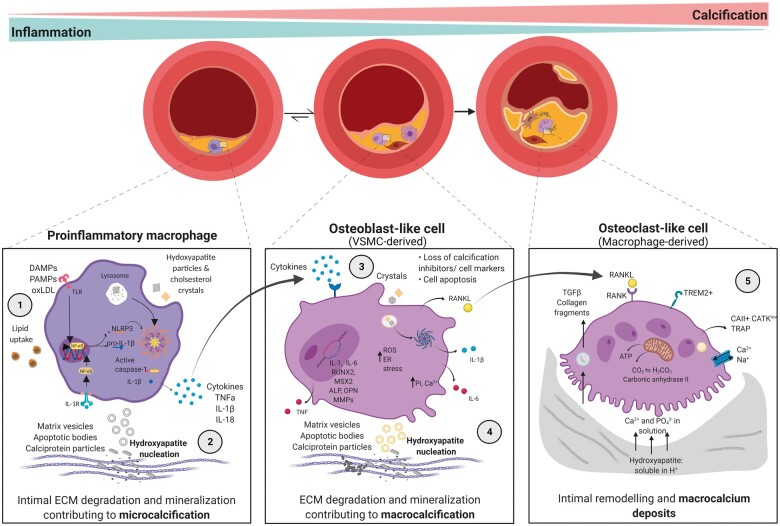
Calcification is an independent predictor of atherosclerosis-related cardiovascular events. Microcalcification is linked to inflamed, unstable lesions, in comparison to the fibrotic stable plaque phenotype generally associated with advanced calcification. This paradox relates to recognition that calcification presents in a wide spectrum of manifestations that differentially impact plaque's fate. Macrophages, the main inflammatory cells in atherosclerotic plaque, have a multifaceted role in disease progression. They crucially control the mineralization process, from microcalcification to the osteoid metaplasia of bone-like tissue. It is a bilateral interaction that weighs heavily on the overall plaque fate but remains rather unexplored. This review highlights current knowledge about macrophage phenotypic changes in relation to and interaction with the calcifying environment. On the one hand, macrophage-led inflammation kickstarts microcalcification through a multitude of interlinked mechanisms, which in turn stimulates phenotypic changes in vascular cell types to drive microcalcification. Macrophages may also modulate the expression/activity of calcification inhibitors and inducers, or eliminate hydroxyapatite nucleation points. Contrarily, direct exposure of macrophages to an early calcifying milieu impacts macrophage phenotype, with repercussions for plaque progression and/or stability. Macrophages surrounding macrocalcification deposits show a more reparative phenotype, modulating extracellular matrix, and expressing osteoclast genes. This phenotypic shift favours gradual displacement of the pro-inflammatory hubs; the lipid necrotic core, by macrocalcification. Parallels to bone metabolism may explain many of these changes to macrophage phenotype, with advanced calcification able to show homeostatic osteoid metaplasia. As the targeted treatment of vascular calcification developing in atherosclerosis is thus far severely lacking, it is crucial to better understand its mechanisms of development.
钙化是动脉粥样硬化相关心血管事件的独立预测因子。与通常与晚期钙化相关的纤维化稳定斑块表型相比,微钙化与炎症性、不稳定病变相关。这种矛盾源于人们认识到钙化存在多种表现形式,这些形式对斑块命运的影响各不相同。巨噬细胞是动脉粥样硬化斑块中的主要炎症细胞,在疾病进展中具有多方面作用。它们在从微钙化到类骨组织骨样化生的矿化过程中起着关键控制作用。这是一种对整体斑块命运有重大影响但仍未得到充分探索的双向相互作用。本综述强调了关于巨噬细胞表型变化及其与钙化环境的关系和相互作用的现有知识。一方面,巨噬细胞主导的炎症通过多种相互关联的机制启动微钙化,进而刺激血管细胞类型的表型变化以推动微钙化。巨噬细胞还可能调节钙化抑制剂和诱导剂的表达/活性,或消除羟基磷灰石成核点。相反,巨噬细胞直接暴露于早期钙化环境会影响巨噬细胞表型,对斑块进展和/或稳定性产生影响。围绕大钙化沉积物的巨噬细胞表现出更具修复性的表型,调节细胞外基质并表达破骨细胞基因。这种表型转变有利于促炎中心逐渐被大钙化取代;脂质坏死核心。与骨代谢的相似之处可能解释了巨噬细胞表型的许多这些变化,晚期钙化能够表现出稳态骨样化生。由于目前严重缺乏针对动脉粥样硬化中发生的血管钙化的靶向治疗,更好地了解其发展机制至关重要。