Division of General Internal Medicine, Department of Medicine, Mayo Clinic, Rochester, MN, USA.
Division of Hematology, Department of Internal Medicine, Mayo Clinic, Rochester, MN, USA.
Blood Cancer J. 2021 Sep 22;11(9):158. doi: 10.1038/s41408-021-00548-7.
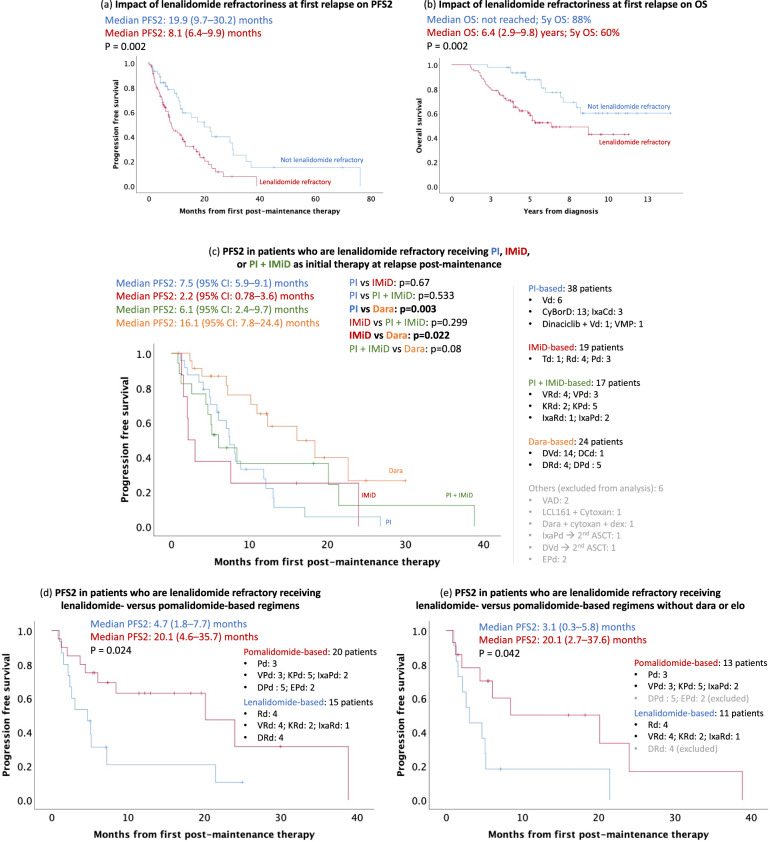
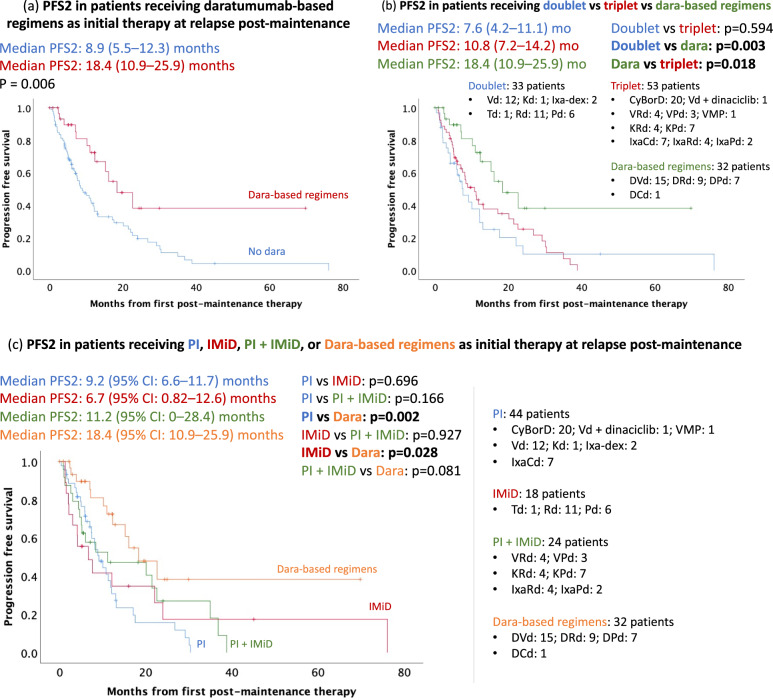
The optimal duration of lenalidomide maintenance post-autologous stem cell transplant (ASCT) in Multiple Myeloma (MM), and choice of therapy at relapse post-maintenance, need further evaluation. This retrospective study assessed outcomes of patients with MM (n = 213) seen at Mayo Clinic, Rochester between 1/1/2005-12/31/2016 who received lenalidomide maintenance post-ASCT. The median PFS was 4 (95% CI: 3.4, 4.5) years from diagnosis of MM; median OS was not reached (5-year OS: 77%). Excluding patients who stopped lenalidomide maintenance within 3 years due to progression on maintenance, ≥3 years of maintenance had a superior 5-year OS of 100% vs. 85% in <3 years (p = 0.011). Median PFS was 7.2 (95% CI: 6, 8.5) years in ≥3 years vs. 4.4 (95% CI: 4.3, 4.5) years in <3 years (p < 0.0001). Lenalidomide refractoriness at first relapse was associated with inferior PFS2 [8.1 (95% CI: 6.4, 9.9) months vs. 19.9 (95% CI: 9.7, 30.2; p = 0.002) months in nonrefractory patients]. At first relapse post-maintenance, median PFS2 was superior with daratumumab-based regimens [18.4 (95% CI: 10.9, 25.9) months] versus regimens without daratumumab [8.9 (95% CI: 5.5, 12.3) months; p = 0.006]. Daratumumab + immunomodulatory drugs had superior median PFS2 compared to daratumumab + bortezomib [NR vs 1 yr (95% CI: 0.5, 1.5); p = 0.004].
在多发性骨髓瘤(MM)中,自体干细胞移植(ASCT)后接受来那度胺维持治疗的最佳持续时间以及维持治疗后复发时的治疗选择需要进一步评估。本回顾性研究评估了 2005 年 1 月 1 日至 2016 年 12 月 31 日在梅奥诊所罗切斯特院区就诊的 213 例 MM 患者的结局;从 MM 诊断开始,中位 PFS 为 4 年(95%CI:3.4,4.5);中位 OS 未达到(5 年 OS:77%)。排除因维持治疗期间进展而在 3 年内停止来那度胺维持治疗的患者,≥3 年的维持治疗 5 年 OS 为 100%,而<3 年的为 85%(p=0.011)。≥3 年的中位 PFS 为 7.2 年(95%CI:6.0,8.5),而<3 年的为 4.4 年(95%CI:4.3,4.5)(p<0.0001)。首次复发时来那度胺耐药与较差的 PFS2 相关[8.1(95%CI:6.4,9.9)个月与非耐药患者的 19.9(95%CI:9.7,30.2;p=0.002)个月]。维持治疗后首次复发时,基于达雷妥尤单抗的方案的中位 PFS2 优于无达雷妥尤单抗的方案[18.4(95%CI:10.9,25.9)个月与 8.9(95%CI:5.5,12.3)个月;p=0.006]。与达雷妥尤单抗+硼替佐米相比,达雷妥尤单抗+免疫调节药物具有更优的中位 PFS2[NR 与 1 年(95%CI:0.5,1.5);p=0.004]。