Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health (DiNOGMI), University of Genoa, Largo Paolo Daneo 3, 16100, Genoa, Italy.
Laboratory of Experimental Neurosciences, IRCCS Ospedale Policlinico San Martino, Genoa, Italy.
Neurotherapeutics. 2021 Oct;18(4):2579-2588. doi: 10.1007/s13311-021-01104-8. Epub 2021 Sep 22.
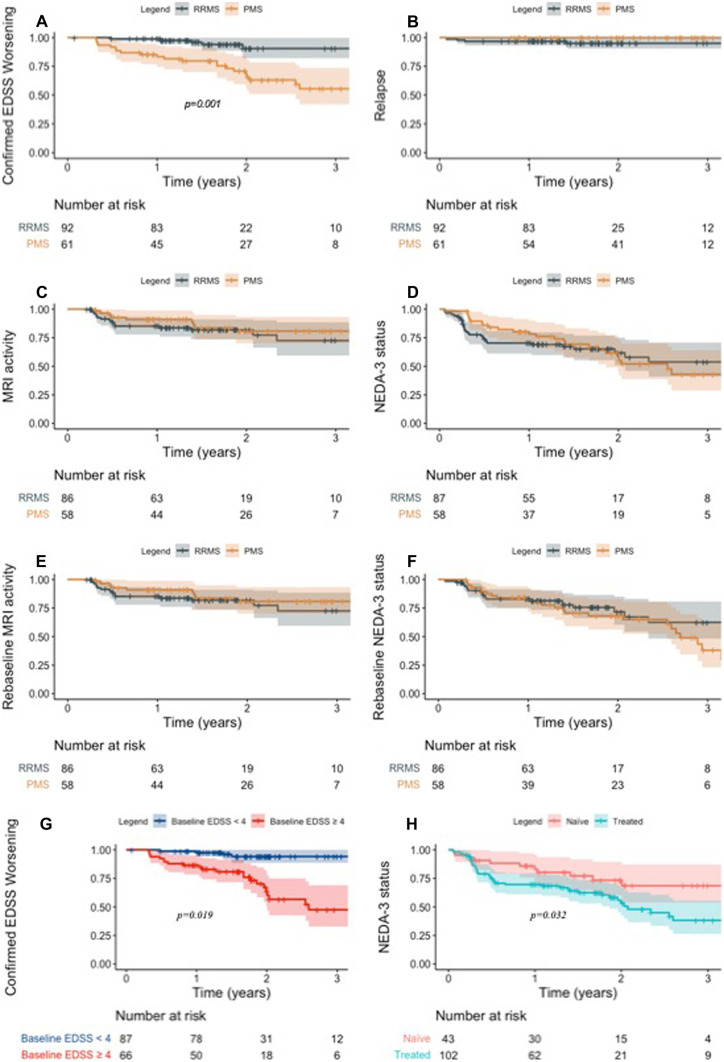
Data regarding effectiveness and safety of ocrelizumab in the post-marking setting are lacking. The aim of our study was to provide effectiveness and safety data of ocrelizumab treatment in patients with relapsing-remitting (RR-) and progressive multiple sclerosis (PMS) and to evaluate clinical and immunological predictors of early treatment response. In this single-center prospective observational study, we investigated effectiveness outcomes (time-to-confirmed disability worsening, time-to-first relapse, time-to-first evidence of MRI activity and time-to-first evidence of disease activity), clinical and immunological predictors of early treatment response, and incidence of adverse events (AEs). One hundred and fifty-three subjects were included (93 RRMS; 84 females). Median follow-up was 1.9 (1.3-2.7). At 2-year follow-up (FU), disability worsening-free survival were 90.5%, 64.7%, and 68.8% for RRMS, primary-progressive MS (PPMS), and secondary-progressive MS (SPMS) patients, respectively. At 2-year FU, 67.1%, 72.7%, and 81.3% of patients with RRMS, PPMS, and SPMS were free of MRI activity, with NEDA-3 percentages of 62.1%, 54.6%, and 55.1%, respectively. Lower baseline EDSS was independently associated with a reduced risk of disability worsening (HR(95%CI) = 1.45(1.05-2.00), p = 0.024) and previous treatment exposure was independently associated with increased probability of radiological activity (HR = 2.53(1.05-6.10), p = 0.039). At 6-month FU, CD8 + cell decrease was less pronounced in patients with inflammatory activity (p = 0.022). Six patients (3.9%) discontinued ocrelizumab due to severe AEs. Our findings suggest that ocrelizumab is an effective treatment in real-world patients with RRMS and PMS, with a manageable safety profile. Better outcomes were observed in treatment-naïve patients and in patients with a low baseline disability level. Depletion of CD8 + cells could underlie early therapeutic effects of ocrelizumab.
关于奥瑞珠单抗在上市后的有效性和安全性的数据尚缺乏。我们的研究旨在提供奥瑞珠单抗治疗复发缓解型(RR)和进展型多发性硬化症(PMS)患者的有效性和安全性数据,并评估早期治疗反应的临床和免疫学预测因素。在这项单中心前瞻性观察性研究中,我们研究了有效性结果(确诊残疾恶化时间、首次复发时间、首次 MRI 活动证据时间和首次疾病活动证据时间)、早期治疗反应的临床和免疫学预测因素以及不良事件(AE)的发生率。共纳入 153 例患者(93 例 RRMS;84 例女性)。中位随访时间为 1.9(1.3-2.7)年。在 2 年随访(FU)时,RRMS、原发性进展型 MS(PPMS)和继发性进展型 MS(SPMS)患者的残疾恶化无进展生存率分别为 90.5%、64.7%和 68.8%。在 2 年 FU 时,67.1%、72.7%和 81.3%的 RRMS、PPMS 和 SPMS 患者无 MRI 活动,NEDA-3 比例分别为 62.1%、54.6%和 55.1%。较低的基线 EDSS 与残疾恶化风险降低独立相关(HR(95%CI)=1.45(1.05-2.00),p=0.024),而先前的治疗暴露与放射学活动的概率增加独立相关(HR=2.53(1.05-6.10),p=0.039)。在 6 个月 FU 时,有炎症活动的患者的 CD8+细胞减少程度较轻(p=0.022)。6 名患者(3.9%)因严重 AE 而停用奥瑞珠单抗。我们的研究结果表明,奥瑞珠单抗在真实世界的 RRMS 和 PMS 患者中是一种有效的治疗方法,具有可管理的安全性。在初治患者和基线残疾水平较低的患者中观察到更好的结果。CD8+细胞的耗竭可能是奥瑞珠单抗早期治疗效果的基础。