From the Barcelonaβeta Brain Research Center (BBRC) (M.M.-A., M.S., G.O., G.S., C.F., J.D.G., N.V.-T., E.M.A.-U., O.G.-R., A.S.-V., G.S.-B., J.M.G.-d-E., C.M., K.F., J.L.M., M.S.-C.), Pasqual Maragall Foundation; IMIM (Hospital del Mar Medical Research Institute) (M.M.-A., M.S., G.O., G.S., C.F., J.D.G., E.M.A.-U., O.G.-R., A.S.-V., G.S.-B., J.M.G.-d-E., C.M., M.S.-C.), Barcelona; Centro de Investigación Biomédica en Red de Fragilidad y Envejecimiento Saludable (CIBERFES) (M.M.-A., G.O., E.M.A.-U., O.G.-R., G.S.-B., C.M., K.F., M.S.-C.), Madrid; Universitat Pompeu Fabra (M.M.-A., M.S.), Barcelona, Spain; Department of Psychiatry and Neurochemistry (A.B., N.J.A., H.K., H.Z., K.B.), Institute of Neuroscience and Physiology, University of Gothenburg; Clinical Neurochemistry Laboratory (A.B., H.K., H.Z., K.B.), Sahlgrenska University Hospital, Mölndal; Wallenberg Centre for Molecular and Translational Medicine (A.B., N.J.A., H.K.), Department of Psychiatry and Neurochemistry, Institute of Neuroscience and Physiology, the Sahlgrenska Academy at the University of Gothenburg, Sweden; King's College London (N.J.A.), Institute of Psychiatry, Psychology & Neuroscience, Maurice Wohl Clinical Neuroscience Institute; NIHR Biomedical Research Centre for Mental Health & Biomedical Research Unit for Dementia at South London & Maudsley NHS Foundation (N.J.A.), London, UK; Centro de Investigación Biomédica en Red de Bioingeniería (C.F., J.D.G., A.N.-B., A.P.), Biomateriales y Nanomedicina (CIBER-BBN), Madrid; Centre for Genomic Regulation (CRG) (N.V.-T.), Barcelona Institute for Science and Technology; Department of Clinical Genetics (N.V.-T.), Erasmus MC, University Medical Center Rotterdam, the Netherlands; Servei de Neurologia (O.G.-R., M.S.-C.), Hospital del Mar; Servei de Medicina Nuclear (A.N.-B., A.P.), Hospital Clínic, Barcelona, Spain; Roche Diagnostics GmbH (G.K.), Penzberg, Germany; Roche Diagnostics International Ltd (I.S.), Rotkreuz, Switzerland; UK Dementia Research Institute at UCL (H.Z.), London; Department of Neurodegenerative Disease (H.Z.), UCL Queen Square Institute of Neurology, London, UK; and H. Lundbeck A/S (J.L.M.), Copenhagen, Denmark.
Neurology. 2021 Nov 23;97(21):e2065-e2078. doi: 10.1212/WNL.0000000000012853. Epub 2021 Sep 23.
To determine whether CSF synaptic biomarkers are altered in the early preclinical stage of the Alzheimer continuum and associated with Alzheimer disease (AD) risk factors, primary pathology, and neurodegeneration markers.
This cross-sectional study was performed in the Alzheimer's and Families (ALFA+) cohort, comprising middle-aged cognitively unimpaired participants. CSF neurogranin and growth-associated protein-43 (GAP-43) were measured with immunoassays, and synaptosomal-associated protein-25 (SNAP-25) and synaptotagmin-1 were measured with immunoprecipitation mass spectrometry. AD CSF biomarkers β-amyloid (Aβ), phosphorylated tau (p-tau), and total tau and the neurodegeneration biomarker neurofilament light chain (NfL) were also measured. Participants underwent structural MRI and fluorodeoxyglucose and Aβ PET imaging. General linear modeling was used to test the associations between CSF synaptic biomarkers and risk factors, Aβ pathology, tau pathology, and neurodegeneration markers.
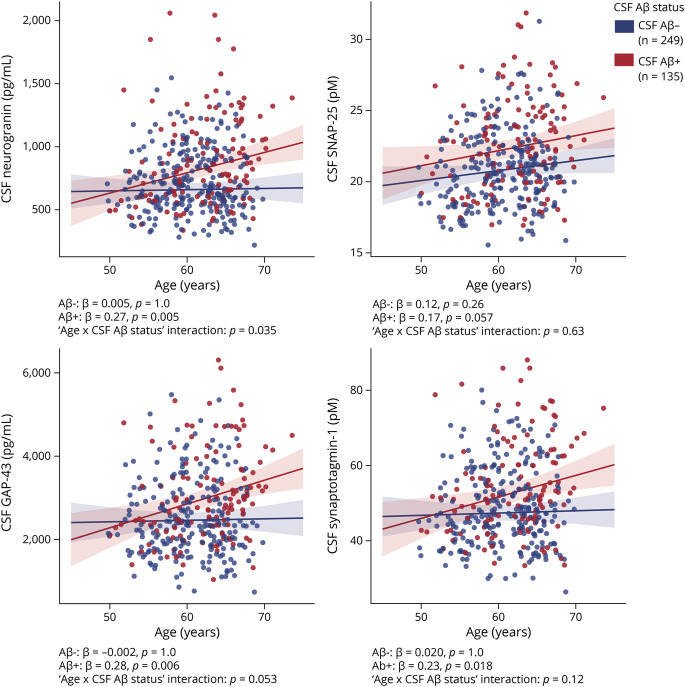
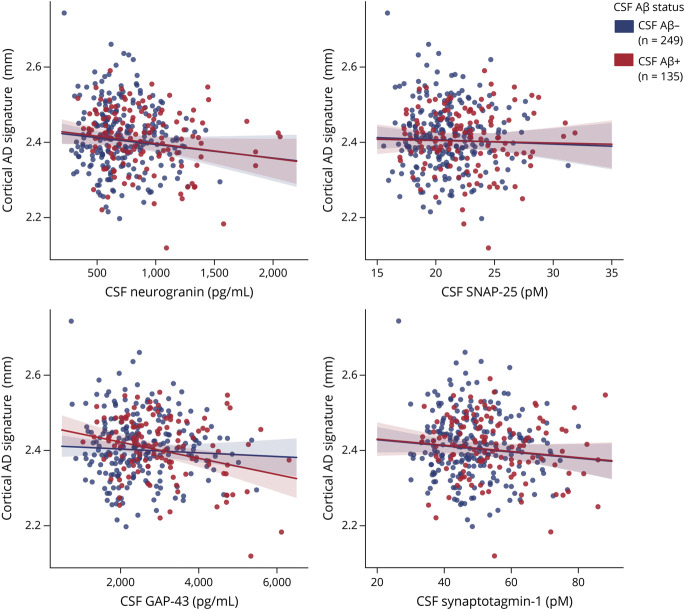
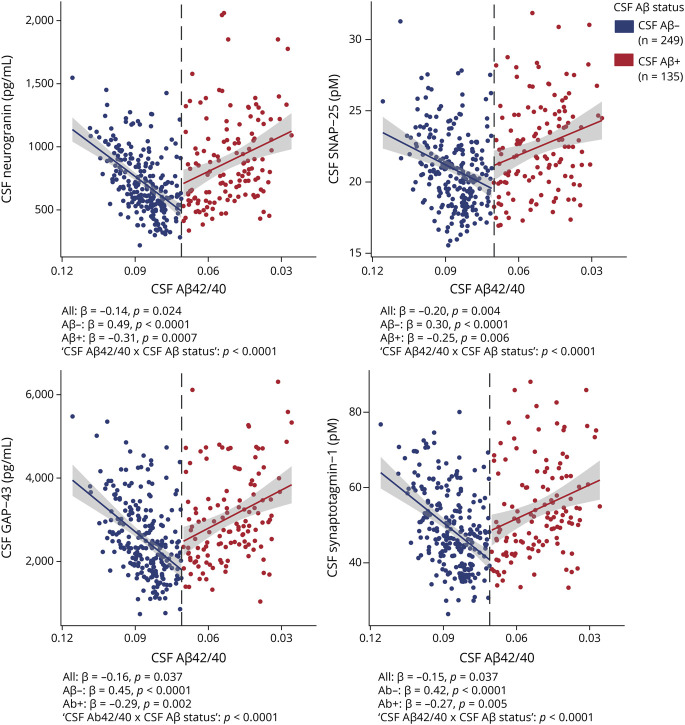
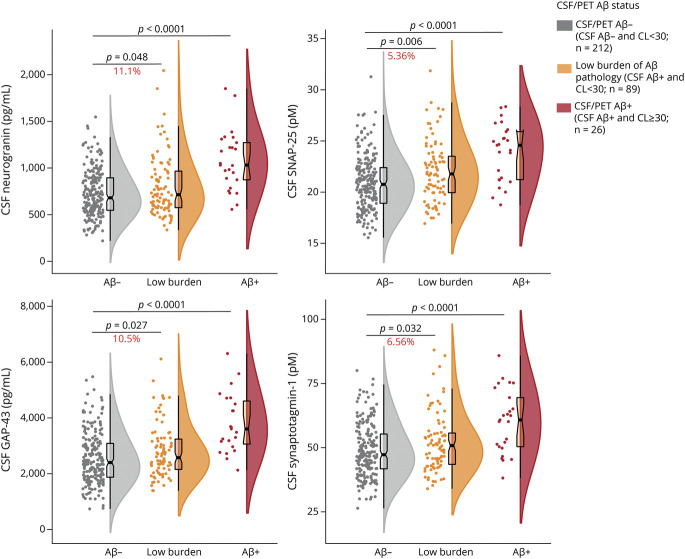
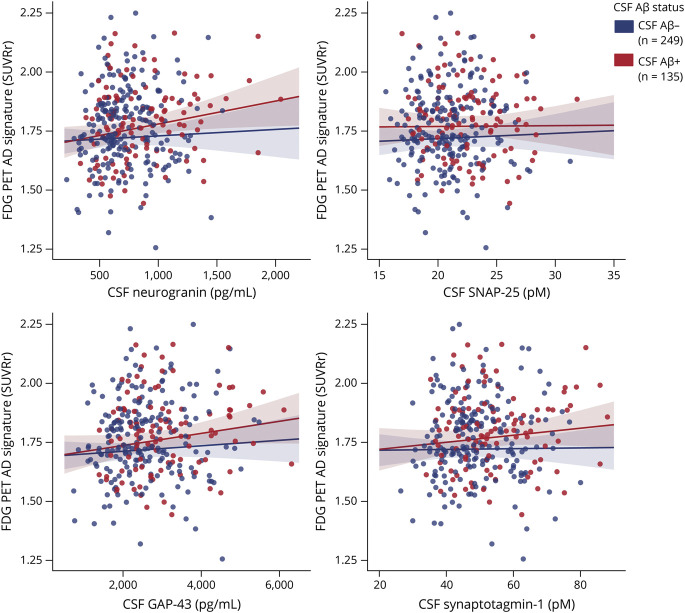
All CSF synaptic biomarkers increased with age. CSF neurogranin was higher in females, while CSF SNAP-25 was higher in ε4 carriers. All CSF synaptic biomarkers increased with higher Aβ load (as measured by CSF Aβ and Aβ PET Centiloid values), and it is important to note that the synaptic biomarkers were increased even in individuals in the earliest stages of Aβ deposition. Higher CSF synaptic biomarkers were also associated with higher CSF p-tau and NfL. Higher CSF neurogranin and GAP-43 were significantly associated with higher brain metabolism but lower cortical thickness in AD-related brain regions.
CSF synaptic biomarkers increase in the early preclinical stages of the Alzheimer continuum even when a low burden of Aβ pathology is present, and they differ in their association with age, sex, ε4 and markers of neurodegeneration.
ClinicalTrials.gov Identifier NCT02485730.
确定 CSF 突触生物标志物是否在阿尔茨海默病连续体的早期临床前阶段发生改变,并与阿尔茨海默病(AD)风险因素、主要病理和神经退行性变标志物相关。
本横断面研究在阿尔茨海默病和家庭(ALFA+)队列中进行,该队列包括中年认知正常的参与者。使用免疫测定法测量 CSF 神经颗粒蛋白和生长相关蛋白-43(GAP-43),使用免疫沉淀质谱法测量突触小体相关蛋白-25(SNAP-25)和突触结合蛋白-1(synaptotagmin-1)。还测量了 AD CSF 生物标志物β-淀粉样蛋白(Aβ)、磷酸化 tau(p-tau)、总 tau 和神经退行性变标志物神经丝轻链(NfL)。参与者接受了结构 MRI 和氟脱氧葡萄糖和 Aβ PET 成像。使用一般线性模型来测试 CSF 突触生物标志物与风险因素、Aβ 病理学、tau 病理学和神经退行性变标志物之间的相关性。
所有 CSF 突触生物标志物均随年龄增长而增加。女性 CSF 神经颗粒蛋白水平较高,而 ε4 携带者 CSF SNAP-25 水平较高。所有 CSF 突触生物标志物均随 Aβ 负荷增加而增加(通过 CSF Aβ 和 Aβ PET Centiloid 值测量),值得注意的是,即使在 Aβ 沉积的最早阶段,突触生物标志物也会增加。较高的 CSF 突触生物标志物也与较高的 CSF p-tau 和 NfL 相关。较高的 CSF 神经颗粒蛋白和 GAP-43 与 AD 相关脑区的脑代谢增加但皮质厚度降低显著相关。
即使在存在低水平 Aβ 病理的情况下,CSF 突触生物标志物也会在阿尔茨海默病连续体的早期临床前阶段增加,并且它们在与年龄、性别、ε4 和神经退行性变标志物的相关性方面存在差异。
ClinicalTrials.gov 标识符 NCT02485730。