Department of Surgery, University of Pittsburgh, Pittsburgh, PA, USA.
Department of Surgery, Epidemiology, Clinical and Translational Science, University of Pittsburgh, Pittsburgh, PA, USA.
Cancer Med. 2021 Oct;10(20):7233-7241. doi: 10.1002/cam4.4211. Epub 2021 Sep 24.
Preoperative autophagy inhibition with hydroxychloroquine (HCQ) in combination with gemcitabine in pancreatic adenocarcinoma (PDAC) has been shown to be safe and effective in inducing a serum biomarker response and increase resection rates in a previous phase I/II clinical trial. We aimed to analyze the long-term outcomes of preoperative HCQ with gemcitabine for this cohort.
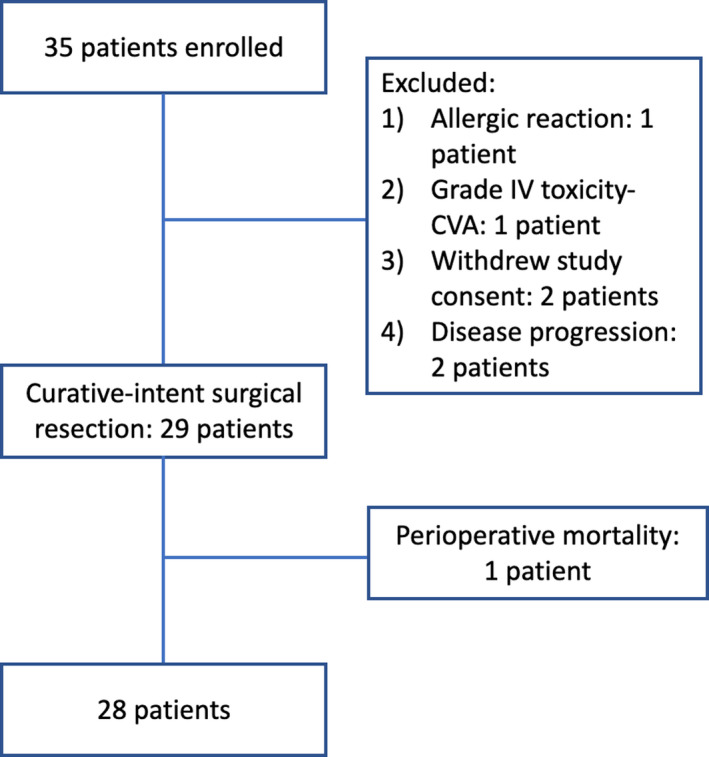
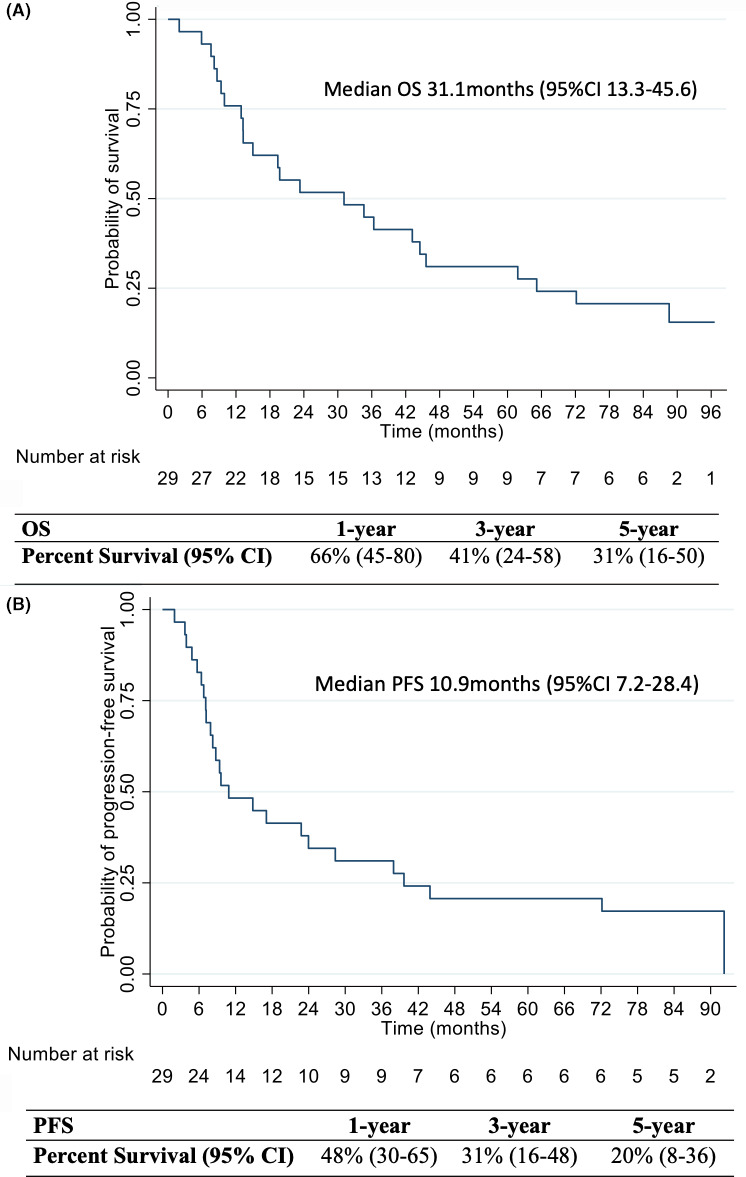
A review of patients enrolled between July 2010 and February 2013 in the completed phase I/II single arm (two doses of fixed-dose gemcitabine (1500 mg/m ) in combination with oral hydroxychloroquine administered for 31 consecutive days until the day of surgery for high-risk pancreatic cancer) was undertaken. Progression-free survival (PFS) and overall survival analysis (OS) using Kaplan-Meier estimates were performed.
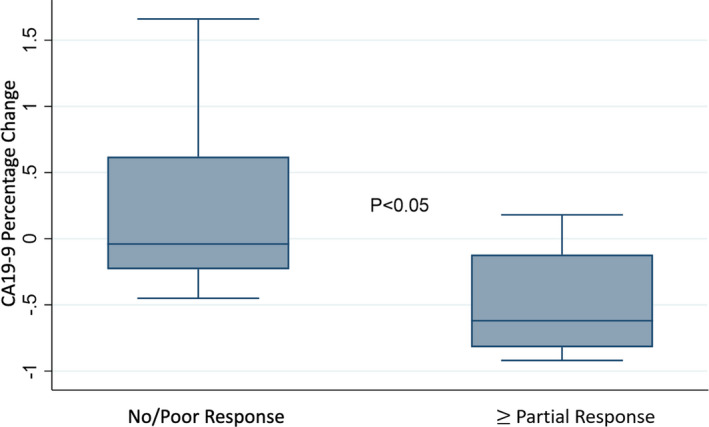
Of 35 patients initially enrolled, 29 patients underwent surgical resection (median age at diagnosis: 62 years, 45% females). Median duration of follow-up was 7.5 years. There was a median 15% decrease in the serum CA19-9 levels following completion of neoadjuvant therapy and 83% of the cohort underwent a pancreaticoduodenectomy, 7 (24%) patients had a concomitant venous resection. On histopathology, 14 (48%) patients had at least a partial treatment response. The median PFS and OS were 11 months (95% Confidence interval [CI]: 7-28) and 31 months (95% CI: 13-47), respectively, while 9 (31%) patients survived beyond 5 years from diagnosis; a rate that compares very favorably with contemporaneous series.
Compared to historical data, neoadjuvant autophagy inhibition with HCQ plus gemcitabine is associated with encouraging long-term survival for patients with PDAC.
在胰腺导管腺癌 (PDAC) 中,术前使用羟氯喹 (HCQ) 联合吉西他滨抑制自噬已被证明在诱导血清生物标志物反应和提高切除率方面是安全有效的,这在前一期 I/II 期临床试验中得到了证实。我们旨在分析这一队列中术前使用 HCQ 联合吉西他滨的长期结果。
对 2010 年 7 月至 2013 年 2 月期间入组的患者进行回顾性分析,该研究为已完成的 I/II 期单臂研究(两种剂量的固定剂量吉西他滨(1500mg/m2)联合口服羟氯喹,连续 31 天,直至手术日,用于高危胰腺癌)。使用 Kaplan-Meier 估计进行无进展生存期 (PFS) 和总生存期 (OS) 分析。
最初入组的 35 例患者中,29 例接受了手术切除(诊断时中位年龄:62 岁,45%为女性)。中位随访时间为 7.5 年。完成新辅助治疗后,血清 CA19-9 水平中位数下降 15%,83%的患者接受了胰十二指肠切除术,7 例(24%)患者同时进行了静脉切除术。在组织病理学上,14 例(48%)患者至少有部分治疗反应。中位 PFS 和 OS 分别为 11 个月(95%置信区间 [CI]:7-28)和 31 个月(95% CI:13-47),9 例(31%)患者从诊断后存活超过 5 年;这一比率与同期系列相比非常有利。
与历史数据相比,PDAC 患者接受 HCQ 联合吉西他滨的自噬抑制新辅助治疗与令人鼓舞的长期生存相关。