Aboubakar Nana Frank, Ocak Sebahat
Institut de Recherche Expérimentale et Clinique (IREC), Pôle de Pneumologie, ORL et Dermatologie (PNEU), Université catholique de Louvain (UCLouvain), 1200 Brussels, Belgium.
Division of Pneumology, Cliniques Universitaires St-Luc, UCLouvain, 1200 Brussels, Belgium.
Pharmaceutics. 2021 Sep 15;13(9):1478. doi: 10.3390/pharmaceutics13091478.
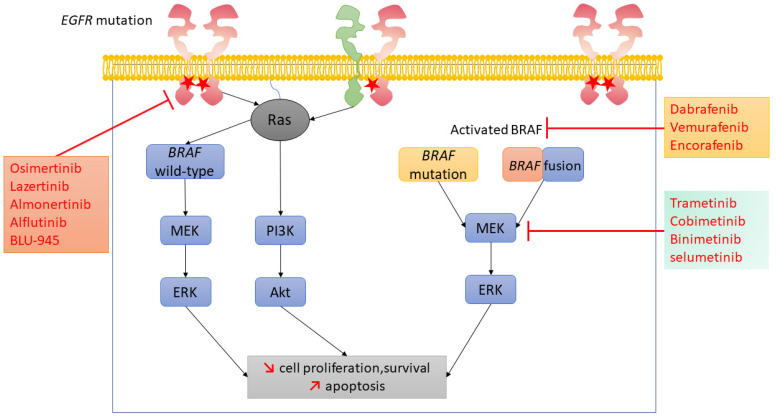
Osimertinib has become a standard of care in the first-line treatment of advanced-stage non-small-cell lung cancer (NSCLC) harboring exon 19 and 21 activating mutations in the gene. Nevertheless, the 18.9-month median progression-free survival emphasizes the fact that resistance to osimertinib therapy is inevitable. Acquired resistance mechanisms to osimertinib in EGFR-driven NSCLC include amplification, C797S mutation, neuroendocrine differentiation, small-cell lung carcinoma histologic transformation, and amplifications and and translocations, as well as V600 mutation. This last one represents 3% of the acquired resistance mechanisms to osimertinib. In this review, we discuss the rationale for EGFR/BRAF/MEK co-inhibition in the light of a clinical case of -mutant NSCLC developing a V600 mutation as an acquired resistance mechanism to osimertinib and responding to the association of osimertinib plus dabrafenib and trametinib. Additionally, we discuss the acquired resistance mechanisms to osimertinib plus dabrafenib and trametinib combination in that context.
奥希替尼已成为携带该基因第19外显子和第21外显子激活突变的晚期非小细胞肺癌(NSCLC)一线治疗的标准疗法。然而,18.9个月的中位无进展生存期凸显了对奥希替尼治疗产生耐药性不可避免这一事实。在EGFR驱动的NSCLC中,奥希替尼获得性耐药机制包括 扩增、C797S突变、神经内分泌分化、小细胞肺癌组织学转化,以及 扩增和 以及 易位,还有V600突变。最后一种情况占奥希替尼获得性耐药机制的3%。在本综述中,我们根据一例 -突变NSCLC发生V600突变作为对奥希替尼的获得性耐药机制并对奥希替尼加达拉非尼和曲美替尼联合用药有反应的临床病例,讨论EGFR/BRAF/MEK联合抑制的基本原理。此外,我们还讨论了在这种情况下奥希替尼加达拉非尼和曲美替尼联合用药的获得性耐药机制。