Alsaeed Meshari, Lim Chloe A R, Plecash Alyson, Chen Tychicus
Division of Neurology, Department of Medicine, University of British Columbia, 2775 Laurel Street, Vancouver, BC, V5Z 1M9, Canada.
Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada.
BMC Neurol. 2021 Sep 27;21(1):374. doi: 10.1186/s12883-021-02404-4.
Paraneoplastic neurologic syndromes (PNS) are rare, however, are important to recognize as oftentimes they precede the detection of an occult malignancy. Our case highlights a rare circumstance of paraneoplastic radiculoneuropathy and the importance of recognizing PNS in antibody negative disease, as is the case in up to 16% of sensory neuronopathies, and the process of excluding other etiologies.
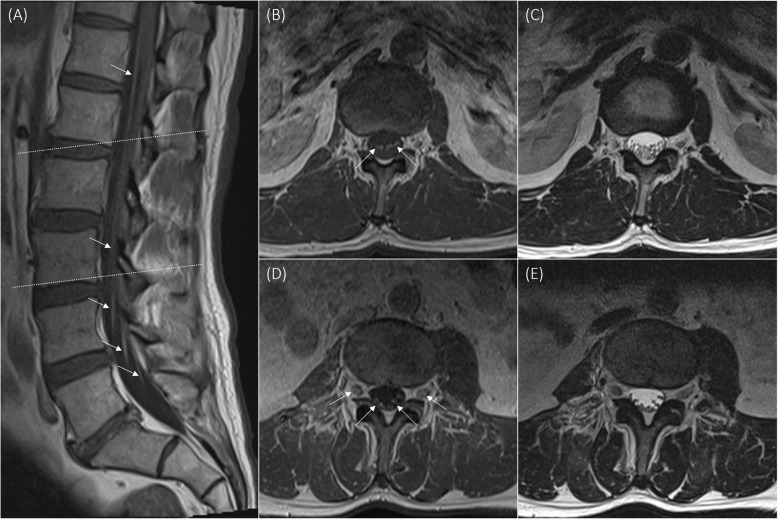
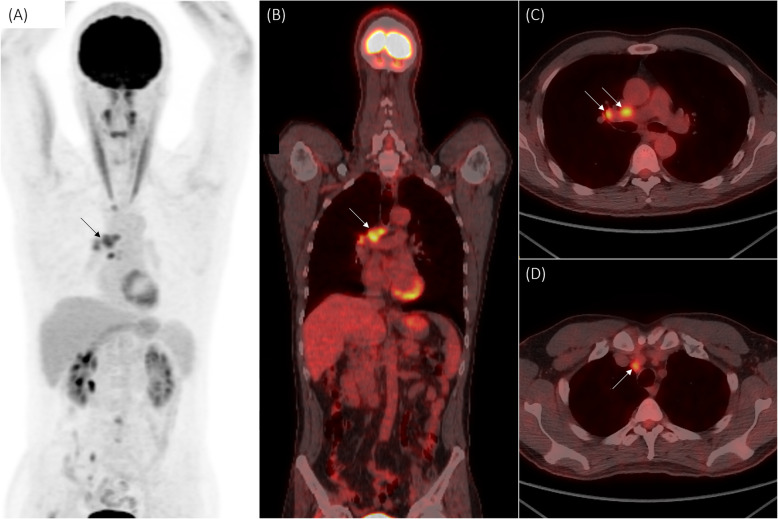
We discuss a 51-year-old man who presented with asymmetric subacute sensorimotor deficits in the lower limbs. Initial clinical examination showed weakness throughout the right lower limb and normal strength on the left with objective numbness in a mixed dermatomal and stocking-glove distribution. Electrophysiology was consistent with axonal sensorimotor neuropathy. Cerebrospinal fluid showed pleocytosis and elevated protein. Intravenous immunoglobulin treatment was given with some improvement in pain symptoms but no measurable motor improvement. Following clinical and electrophysiologic deterioration the patient was transferred to a tertiary centre. Magnetic resonance imaging of the spine showed smooth enhancement of the ventral caudal nerve roots. Chest computed tomography revealed left lower vascular scarring. Further positron emission tomography scan imaging identified fluorodeoxyglucose avid right lung lymphadenopathy. Bronchoscopy-guided biopsy revealed small cell lung carcinoma. Onconeural and antiganglioside antibodies were negative. The patient was then transferred to a medical oncology ward where he underwent chemoradiotherapy and subsequently experienced improvement in his motor function, supporting that his neurological condition was indeed secondary to a paraneoplastic process.
Onconeural negative paraneoplastic radiculoneuropathy can precede diagnosis of small cell lung carcinoma. If considered early and adequately investigated, it can allow earlier diagnosis and treatment of underlying malignancy, improving overall and neurological prognosis.
副肿瘤性神经系统综合征(PNS)较为罕见,但因其常先于隐匿性恶性肿瘤的发现而具有重要的识别意义。我们的病例突出了副肿瘤性神经根神经病这一罕见情况,以及在抗体阴性疾病(如高达16%的感觉神经元病)中识别PNS的重要性,还有排除其他病因的过程。
我们讨论一名51岁男性,其出现下肢不对称性亚急性感觉运动功能障碍。初始临床检查显示右下肢肌力减弱,左下肢肌力正常,伴有混合性皮节和手套袜套样分布的客观麻木感。电生理检查结果符合轴索性感觉运动神经病。脑脊液检查显示有细胞增多和蛋白升高。给予静脉注射免疫球蛋白治疗后,疼痛症状有所改善,但运动功能无明显改善。随着临床和电生理状况恶化,患者被转至三级中心。脊柱磁共振成像显示尾侧腹侧神经根有光滑强化。胸部计算机断层扫描显示左下肺血管瘢痕形成。进一步的正电子发射断层扫描成像发现右肺淋巴结有氟脱氧葡萄糖摄取增加。支气管镜引导下活检显示为小细胞肺癌。肿瘤相关神经元抗体和抗神经节苷脂抗体均为阴性。随后患者被转至肿瘤内科病房,在那里接受了放化疗,其运动功能随后有所改善,这支持了其神经状况确实继发于副肿瘤过程。
肿瘤相关神经元抗体阴性的副肿瘤性神经根神经病可先于小细胞肺癌的诊断出现。如果早期考虑并进行充分检查,可实现潜在恶性肿瘤的早期诊断和治疗,改善总体预后和神经预后。