Department of Urology, Comprehensive Cancer Center, Medical University of Vienna, Vienna, Austria.
Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia.
Mol Carcinog. 2022 Jan;61(1):5-18. doi: 10.1002/mc.23355. Epub 2021 Sep 29.
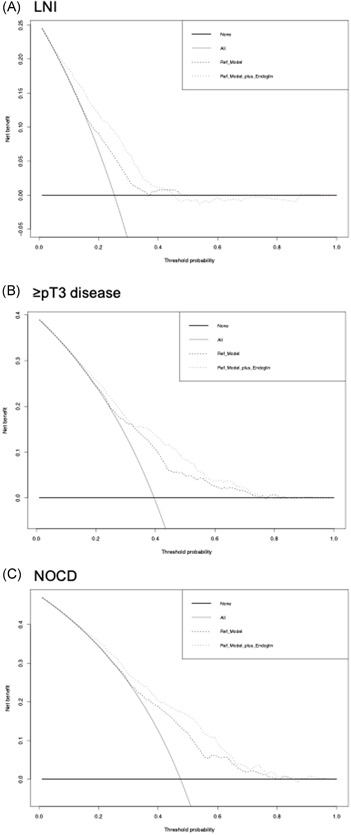
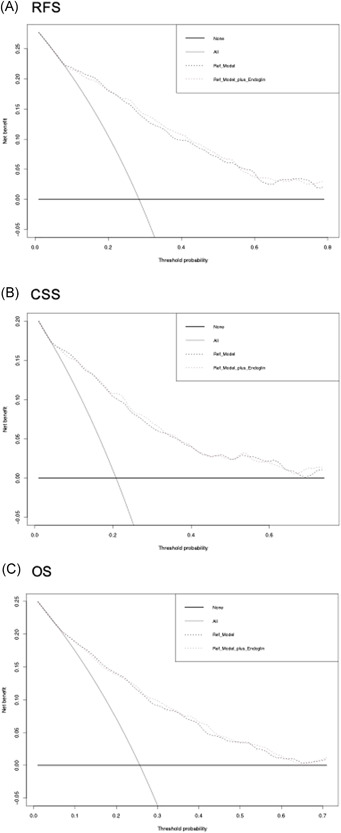
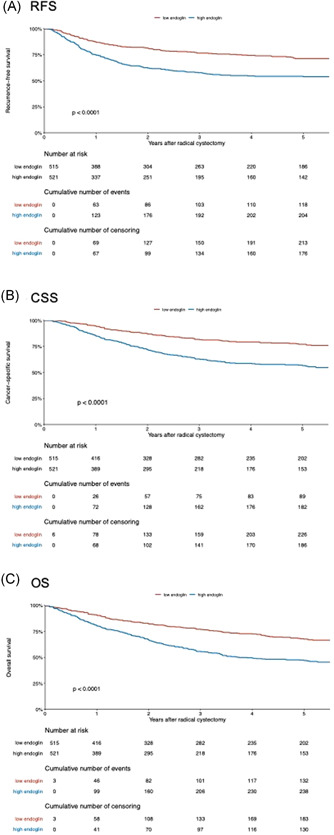
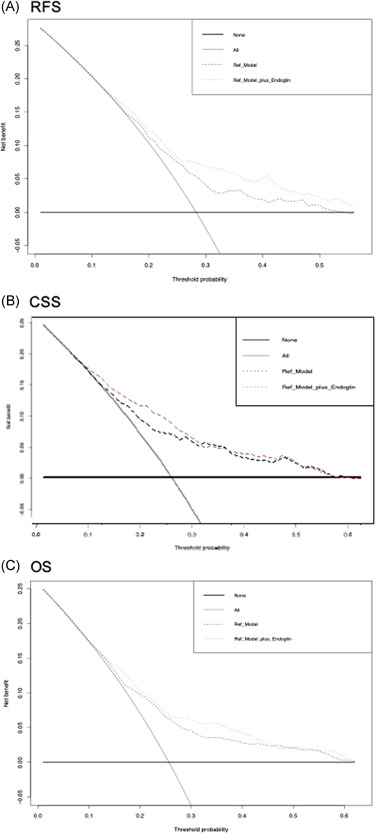
Elevated preoperative plasma level of endoglin has been associated with worse oncologic outcomes in various malignancies. The present large-scale study aimed to determine the predictive and prognostic values of preoperative endoglin with regard to clinicopathologic and survival outcomes in patients treated with radical cystectomy (RC) for nonmetastatic urothelial carcinoma of the bladder (UCB). We prospectively collected preoperative blood samples from 1036 consecutive patients treated with RC for UCB. Logistic and Cox regression analyses were undertaken to assess the correlation of endoglin levels with pathologic and survival outcomes, respectively. The AUC and C-index were used to assess the discrimination. Patients with adverse pathologic features had significantly higher median preoperative endoglin plasma levels than their counterparts. Higher preoperative endoglin level was independently associated with an increased risk for lymph node metastasis, ≥pT3 disease, and nonorgan confined disease (NOCD; all p < 0.001). Plasma endoglin level was also independently associated with cancer-specific and overall survival in both pre- and postoperative models (all p < 0.05), as well as with recurrence-free survival (RFS) in the preoperative model (p < 0.001). The addition of endoglin to the preoperative standard model improved its discrimination for prediction of lymph node metastasis, ≥pT3 disease, NOCD, and RFS (differential increases in C-indices: 10%, 5%, 5.8%, and 4%, respectively). Preoperative plasma endoglin is associated with features of biologically and clinically aggressive UCB as well as survival outcomes. Therefore, it seems to hold the potential of identifying UCB patients who may benefit from intensified therapy in addition to RC such as extended lymphadenectomy or/and preoperative systemic therapy.
术前血浆内皮糖蛋白水平升高与多种恶性肿瘤的肿瘤学预后不良相关。本大规模研究旨在确定术前内皮糖蛋白对接受根治性膀胱切除术(RC)治疗非转移性膀胱癌(UCB)患者的临床病理和生存结局的预测和预后价值。我们前瞻性地收集了 1036 例接受 RC 治疗 UCB 的连续患者的术前血液样本。逻辑和 Cox 回归分析分别用于评估内皮糖蛋白水平与病理和生存结局的相关性。AUC 和 C 指数用于评估鉴别力。具有不良病理特征的患者术前内皮糖蛋白血浆水平中位数明显高于对照组。术前内皮糖蛋白水平升高与淋巴结转移、≥pT3 疾病和非器官受限疾病(NOCD;均 p<0.001)的风险增加独立相关。在术前和术后模型中,血浆内皮糖蛋白水平也与癌症特异性和总生存相关(均 p<0.05),以及与术前模型中的无复发生存(RFS)相关(p<0.001)。将内皮糖蛋白添加到术前标准模型中可以提高其对预测淋巴结转移、≥pT3 疾病、NOCD 和 RFS 的鉴别力(C 指数差异增加:10%、5%、5.8%和 4%,分别)。术前血浆内皮糖蛋白与生物学和临床侵袭性 UCB 的特征以及生存结局相关。因此,它似乎有潜力识别可能从 RC 以外的强化治疗中获益的 UCB 患者,例如扩大淋巴结切除术或/和术前全身治疗。