Robinson-Papp Jessica, Astha Varuna, Nmashie Alexandra, Sharma Sandeep K, Kim-Schulze Seunghee, Murray Jacinta, George Mary Catherine, Morgello Susan, Mueller Bridget R, Lawrence Steven A, Benn Emma K T
Icahn School of Medicine at Mount Sinai, Department of Neurology, United States.
Icahn School of Medicine at Mount Sinai, Center for Scientific Diversity, Center for Biostatistics & Department of Population Health Science and Policy, United States.
Brain Behav Immun Health. 2020 Aug 3;7:100112. doi: 10.1016/j.bbih.2020.100112. eCollection 2020 Aug.
HIV-associated autonomic neuropathy (HIV-AN) is common and may be associated with both sympathetic and parasympathetic dysfunction. Sympathetic nervous system (SNS) dysfunction occurs on a continuum of hyper-to hypo-adrenergic function, and may be a mediator between psychological stress and chronic inflammation. We sought to describe patterns of SNS dysfunction in people living with HIV, and to determine whether SNS dysfunction is associated with markers of systemic inflammation (focusing on IL-6 and TNF-α) and pain and anxiety.
Forty-seven people with well-controlled HIV and without confounding medical conditions or medications completed the Medical Outcomes Survey (MOS-HIV), quantification of a panel of 41 plasma cytokines/chemokines, and a standardized, non-invasive autonomic reflex screen (ARS). Adrenergic baroreflex sensitivity (BRSA) was calculated from the ARS as a measure of SNS function.
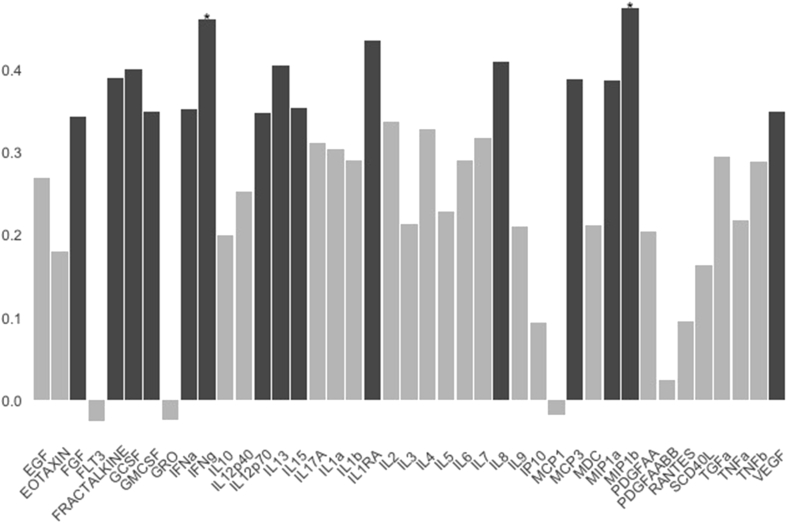
Pain (46%) and anxiety (52%) were commonly reported on the MOS-HIV. BRSA was reduced in 30% of participants and elevated in 9% with the latter occurring only in participants with normal to mild HIV-AN. BRSA was significantly associated with IL-6, but not with TNF-α, pain or anxiety. Exploratory analyses also revealed positive associations of BRSA with numerous other cytokines with no significant inverse associations.
Higher BRSA, indicative of a more hyperadrenergic state, can be part of the spectrum of early HIV-AN, and may be associated with elevations in multiple cytokines including IL-6. These associations do not appear to be driven by stressors such as pain or anxiety.
人类免疫缺陷病毒相关自主神经病变(HIV-AN)很常见,可能与交感神经和副交感神经功能障碍均有关。交感神经系统(SNS)功能障碍在高肾上腺素能到低肾上腺素能功能的连续体上发生,可能是心理压力和慢性炎症之间的介质。我们试图描述HIV感染者中SNS功能障碍的模式,并确定SNS功能障碍是否与全身炎症标志物(重点关注白细胞介素-6和肿瘤坏死因子-α)以及疼痛和焦虑相关。
47名HIV病情得到良好控制、无混杂医疗状况或药物治疗的患者完成了医疗结果调查(MOS-HIV)、41种血浆细胞因子/趋化因子的定量检测以及标准化的非侵入性自主神经反射筛查(ARS)。从ARS计算肾上腺素能压力反射敏感性(BRSA)作为SNS功能的指标。
在MOS-HIV中,疼痛(46%)和焦虑(52%)很常见。30%的参与者BRSA降低,9%的参与者BRSA升高,后者仅发生在HIV-AN正常至轻度的参与者中。BRSA与白细胞介素-6显著相关,但与肿瘤坏死因子-α、疼痛或焦虑无关。探索性分析还显示BRSA与许多其他细胞因子呈正相关,无显著负相关。
较高的BRSA表明处于高肾上腺素能状态,可能是早期HIV-AN谱的一部分,可能与包括白细胞介素-6在内的多种细胞因子升高有关。这些关联似乎不是由疼痛或焦虑等应激源驱动的。