Shinno Yuki, Goto Yasushi, Ohuchi Mayu, Hamada Akinobu, Nokihara Hiroshi, Fujiwara Yasuhiro, Ohe Yuichiro
Department of Thoracic Oncology, National Cancer Center Hospital, Tsukiji, Chuo-ku, Tokyo, Japan.
Division of Molecular Pharmacology, Exploratory Oncology Research and Clinical Trial Center, National Cancer Center, Tsukiji, Chuo-ku, Tokyo, Japan.
JTO Clin Res Rep. 2020 Feb 11;1(1):100008. doi: 10.1016/j.jtocrr.2020.100008. eCollection 2020 Mar.
EGFR tyrosine kinase inhibitors are one of the key drugs for treatment of NSCLC with mutations. In recent times, immune check-point inhibitors (ICIs) have also been widely used for patients with NSCLC. Although a subset of patients obtain benefit from ICIs, adverse events (AEs) that are different from those of cytotoxic chemotherapies may occur. Moreover, some patients develop AEs, which seem to be caused by the previously discontinued nivolumab.
We identified patients with NSCLC who developed AEs, which started shortly after discontinuation of nivolumab and during treatment with osimertinib. We conducted liquid chromatography-mass spectrometry analyses to estimate the concentration of serum nivolumab.
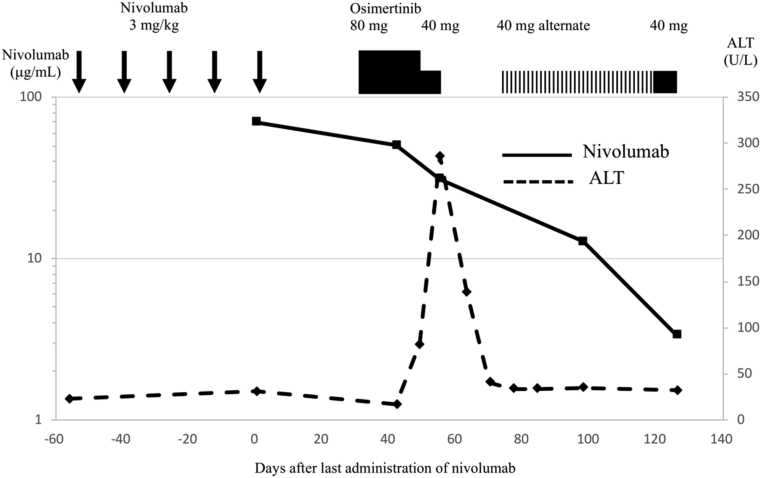
Three patients with AEs were identified. Two patients developed interstitial lung disease (cases 1 and 2) and one developed hepatotoxicity (case 3) during osimertinib therapy initiated after nivolumab administration. They received several treatments, including cytotoxic chemotherapies or EGFR tyrosine kinase inhibitors other than osimertinib, followed by nivolumab for three to five cycles; nevertheless, the disease progressed. After discontinuation of nivolumab, osimertinib was administered from day 22 to 46; but treatment-related toxicities developed 56 to 96 days later. Liquid chromatography-mass spectrometry analyses revealed that the remaining levels of nivolumab in the blood (2.1 μg/mL, 12.8 μg/mL, and 31.1 μg/mL, respectively, for cases 1, 2, and 3) were enough to induce an immune response.
The presence of the ICI antibody that persists even after drug discontinuation may account not only for the prolonged efficacy of these agents but also for the late onset of AEs, especially when the antibodies may have interacted during subsequent treatments.
表皮生长因子受体(EGFR)酪氨酸激酶抑制剂是治疗具有特定突变的非小细胞肺癌(NSCLC)的关键药物之一。近年来,免疫检查点抑制剂(ICI)也已广泛应用于NSCLC患者。尽管一部分患者从ICI中获益,但可能会出现与细胞毒性化疗不同的不良事件(AE)。此外,一些患者出现的AE似乎是由先前停用的纳武单抗引起的。
我们确定了在停用纳武单抗后不久且在使用奥希替尼治疗期间出现AE的NSCLC患者。我们进行了液相色谱 - 质谱分析以估计血清纳武单抗的浓度。
确定了3例出现AE的患者。在纳武单抗给药后开始的奥希替尼治疗期间,2例患者出现间质性肺病(病例1和2),1例出现肝毒性(病例3)。他们接受了多种治疗,包括细胞毒性化疗或除奥希替尼之外的EGFR酪氨酸激酶抑制剂,随后接受了三到五个周期的纳武单抗治疗;然而,疾病仍进展。停用纳武单抗后,从第22天至46天给予奥希替尼;但在56至96天后出现了与治疗相关的毒性。液相色谱 - 质谱分析显示,血液中纳武单抗的剩余水平(病例1、2和3分别为2.1μg/mL、12.8μg/mL和31.1μg/mL)足以诱导免疫反应。
即使在停药后仍持续存在的ICI抗体不仅可能导致这些药物疗效延长,还可能导致AE的迟发,特别是当这些抗体在后续治疗期间可能发生相互作用时。