Hepatobiliary Surgery and Liver Transplantation, University of Pisa Medical School Hospital, Pisa, Italy.
Intensive Care Unit, University of Pisa Medical School Hospital, Pisa, Italy.
Surg Endosc. 2022 May;36(5):3317-3322. doi: 10.1007/s00464-021-08645-1. Epub 2021 Oct 4.
Preliminary experience in laparoscopic liver surgery is usually suggested prior to implementation of a robotic liver resection program.
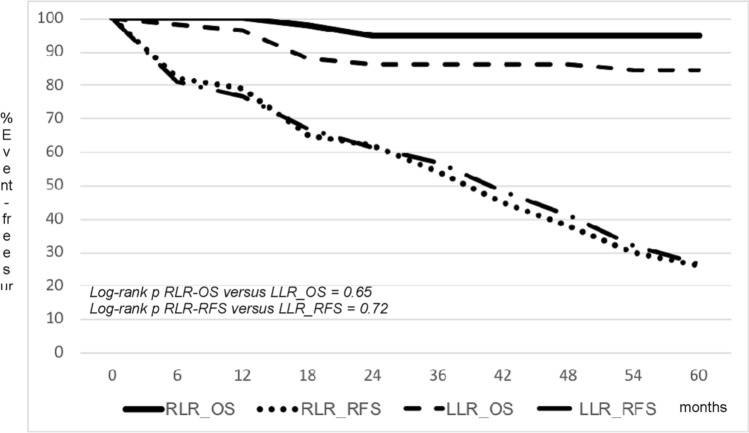
This was a retrospective cohort analysis of patients undergoing robotic (RLR) versus laparoscopic liver resection (LLR) for hepatocellular carcinoma at a center with concomitant initiation of robotic and laparoscopic programs RESULTS: A total of 92 consecutive patients operated on between May 2014 and February 2019 were included: 40 RLR versus 52 LLR. Median age (69 vs. 67; p = 0.74), male sex (62.5% vs. 59.6%; p = 0.96), incidence of chronic liver disease (97.5% vs.98.1%; p = 0.85), median model for end-stage liver disease (MELD) score (8 vs. 9; p = 0.92), and median largest nodule size (22 vs. 24 mm) were similar between RLR and LLR. In the LLR group, there was a numerically higher incidence of nodules located in segment 4 (20.0% vs. 16.6%; p = 0.79); a numerically higher use of Pringle's maneuver (32.7% vs. 20%; p = 0.23), and a shorter duration of surgery (median of 165.5 vs. 217.5 min; p = 0.04). Incidence of complications (25% vs.32.7%; p = 0.49), blood transfusions (2.5% vs.9.6%; p = 0.21), and median length of stay (6 vs. 5; p = 0.54) were similar between RLR and LLR. The overall (OS) and recurrence-free (RFS) survival rates at 1 and 5 years were 100 and 79 and 95 and 26% for RLR versus 96.2 and 76.9 and 84.6 and 26.9% for LLR (log-rank p = 0.65 for OS and 0.72 for RFS).
Based on our results, concurrent implementation of a robotic and laparoscopic liver resection program appears feasible and safe, and is associated with similar oncologic long-term outcomes.
在实施机器人肝切除术计划之前,通常建议先进行腹腔镜肝手术的初步经验。
这是一项回顾性队列分析,纳入了 2014 年 5 月至 2019 年 2 月在一个中心接受机器人(RLR)与腹腔镜肝切除术(LLR)治疗肝细胞癌的患者,该中心同时开展了机器人和腹腔镜项目。
共纳入 92 例连续患者:40 例 RLR 与 52 例 LLR。中位年龄(69 岁比 67 岁;p=0.74)、男性比例(62.5%比 59.6%;p=0.96)、慢性肝病发生率(97.5%比 98.1%;p=0.85)、中位终末期肝病模型(MELD)评分(8 分比 9 分;p=0.92)和最大肿瘤直径(22 毫米比 24 毫米)在 RLR 和 LLR 之间相似。在 LLR 组中,位于第 4 段的肿瘤比例较高(20.0%比 16.6%;p=0.79),普雷尔氏手法(Pringle's maneuver)的使用率较高(32.7%比 20%;p=0.23),手术时间较短(中位数 165.5 分钟比 217.5 分钟;p=0.04)。并发症发生率(25%比 32.7%;p=0.49)、输血率(2.5%比 9.6%;p=0.21)和中位住院时间(6 天比 5 天;p=0.54)在 RLR 和 LLR 之间相似。1 年和 5 年的总体生存率(OS)和无复发生存率(RFS)分别为 100%和 79%,95%和 26%,用于 RLR,96.2%和 76.9%,84.6%和 26.9%,用于 LLR(对数秩检验,OS 为 p=0.65,RFS 为 p=0.72)。
根据我们的结果,同时开展机器人和腹腔镜肝切除术计划是可行和安全的,并且与相似的肿瘤学长期结果相关。