Bernardi Lorenzo, Balzano Emanuele, Roesel Raffaello, Senatore Annamaria, Pezzati Daniele, Catalano Gabriele, Garo Maria Luisa, Tincani Giovanni, Majno-Hurst Pietro, Ghinolfi Davide, Cristaudi Alessandra
Department of Surgery, Lugano Regional Hospital, Ente Ospedaliero Cantonale (EOC), Via Tesserete 46, 6900, Lugano, Switzerland.
Hepato-Biliary Surgery and Liver Transplant Division, Azienda Ospedaliera Universitaria Pisana (AOUP), University of Pisa, Via Paradisa, 2, 56124, Pisa, Italy.
Surg Endosc. 2025 Mar;39(3):2116-2128. doi: 10.1007/s00464-025-11553-3. Epub 2025 Feb 4.
Robotic (RLR) and laparoscopic liver resection (LLR) for hepatocellular carcinoma (HCC) provide similar short-term outcomes, but data focused on recurrence and survival are still lacking. We hypothesized non-inferior oncologic results of RLR compared to LLR for HCC of stage BCLC 0-A.
RLRs and LLRs on patients with HCC of stage BCLC 0-A and preserved liver function (Child A or B if cirrhosis) were retrospectively reviewed. Propensity score matching (PSM) was used to mitigate selection bias. The primary endpoints were recurrence-free (RFS) and overall survival (OS); secondary endpoints were incidence, pattern, and treatment of recurrences.
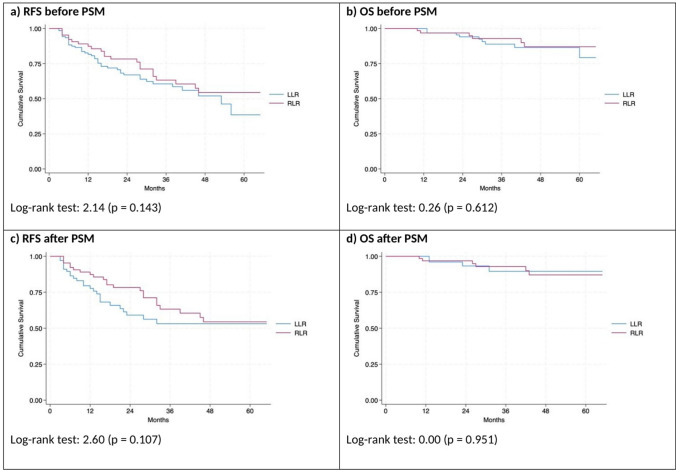
After 1:1 PSM, two groups (RLR = 68; LLR = 68) of patients with similar characteristics, liver function and HCC features were obtained: median age 71-years, males 73.5%, underlying cirrhosis 91.2% (Child A, 96.8%, MELD ≤ 9, 96.0%), portal hypertension 22.1%, single-HCC 90.4%. Two- and 5-year RFS were 78.0 vs 59.0% and 54.0 vs 53.0% (p = 0.107), while OS was 97.0 vs 90.0% and 87.0 vs 90.0% (p = 0.951) for RLR vs LLR, respectively. Incidence of HCC recurrence was similar (35.3 vs 39.7%; p = 0.723). Recurrences developed mostly within the liver (29.4 vs 30.9%; p = 1.000) and within 2 years after hepatectomy (19.1 vs 32.4%, p = 0.116) in RLR vs LLRs. Curative-intent treatment of recurrences did not differ (liver transplantation 19.6%, redo-resection 15.7%, locoregional treatments 52.9%) except for a tendency toward more redo-resections for recurrences after RLR.
Oncologic outcomes of RLR were not inferior to those of LLR in selected HCC patients of stage BCLC 0-A with underlying cirrhosis. Both techniques guaranteed similar salvageability in case of HCC recurrence.
机器人肝切除术(RLR)和腹腔镜肝切除术(LLR)治疗肝细胞癌(HCC)的短期疗效相似,但仍缺乏关于复发和生存的数据。我们假设对于BCLC 0-A期HCC,RLR的肿瘤学结果不劣于LLR。
回顾性分析BCLC 0-A期HCC且肝功能保留(若有肝硬化则为Child A或B级)患者的RLR和LLR情况。采用倾向评分匹配(PSM)以减轻选择偏倚。主要终点为无复发生存期(RFS)和总生存期(OS);次要终点为复发的发生率、模式和治疗。
经过1:1 PSM后,获得了两组(RLR = 68例;LLR = 68例)具有相似特征、肝功能和HCC特征的患者:中位年龄71岁,男性占73.5%,潜在肝硬化占91.2%(Child A级占96.8%,终末期肝病模型评分(MELD)≤9分占96.0%),门静脉高压占22.1%,单发HCC占90.4%。RLR组与LLR组的2年和5年RFS分别为78.0%对59.0%和54.0%对53.0%(p = 0.107),而OS分别为97.0%对90.0%和87.0%对90.0%(p = 0.951)。HCC复发的发生率相似(35.3%对39.7%;p = 0.723)。RLR组与LLR组相比,复发大多发生在肝内(29.4%对30.9%;p = 1.000)且在肝切除术后2年内(19.1%对32.4%,p = 0.116)。除RLR术后复发进行再次手术切除的趋势更大外,复发的根治性治疗无差异(肝移植19.6%,再次手术切除15.7%,局部治疗52.9%)。
对于有潜在肝硬化的BCLC 0-A期特定HCC患者,RLR的肿瘤学结果不劣于LLR。在HCC复发的情况下,两种技术保证了相似的挽救性。