Department of Blood Transfusion, The Second Xiangya Hospital of Central South University, Changsha, China.
Department of Cardiovascular Medicine, The Second Xiangya Hospital of Central South University, No. 139, Middle Renmin Road, Changsha, 410011, Hunan, People's Republic of China.
Cardiovasc Diabetol. 2021 Oct 5;20(1):201. doi: 10.1186/s12933-021-01393-5.
Previous studies reported the prognostic value of the atherogenic index of plasma (AIP) in the course of atherosclerosis and other cardiovascular diseases (CVDs). Still, the predictive utility of the AIP is unknown among patients with type 2 diabetes mellitus (T2DM).
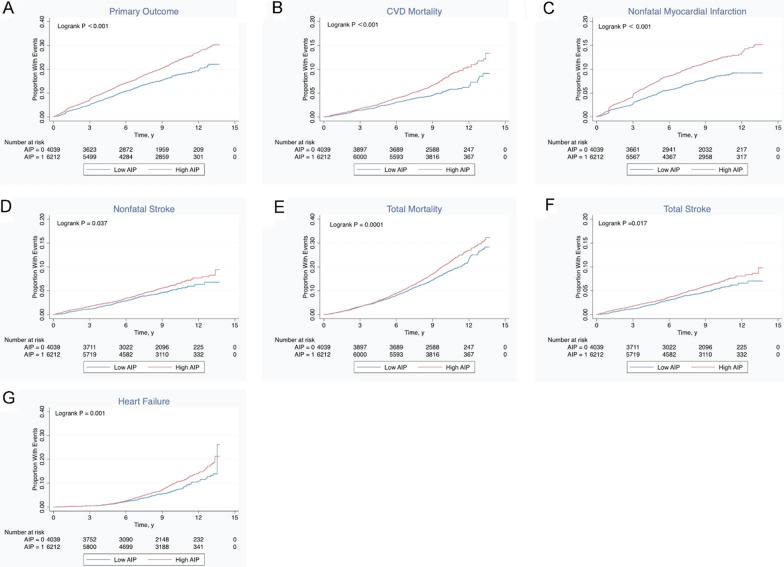
This was a secondary analysis of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) study, which randomized 10,251 patients with long-lasting T2DM. ROC curve analysis was used to determine an optimal threshold for AIP, and the study population was divided into high and low AIP groups. Univariable and multivariable Cox proportional hazards regression analyses were used to determine the association between AIP and primary (major adverse cardiovascular events [MACEs], including nonfatal myocardial infarction, nonfatal stroke, and/or death from cardiovascular causes) and secondary outcomes (all-cause mortality). Stratified analyses were performed to control for the confounding factors.
AIP was an independent risk factor for the prognosis of T2DM (HR = 1.309; 95% CI 1.084-1.581; P = 0.005). The threshold for AIP was determined to be 0.34 in the study population. After adjustments for confounding factors, multivariable analysis showed that AIP was associated with the risk of MACEs (Model 1: HR = 1.333, 95% CI 1.205-1.474, P < 0.001; Model 2: HR = 1.171, 95% CI 1.030-1.333, P = 0.016; Model 3: HR = 1.194, 95% CI 1.049-1.360, P = 0.007), all-cause mortality (Model 1: HR = 1.184, 95% CI 1.077-1.303, P < 0.001), cardiovascular death (Model 1: HR = 1.422, 95% CI 1.201-1.683, P < 0.001; Model 3: HR = 1.264, 95% CI 1.015-1.573, P = 0.036), and nonfatal myocardial infarction (Model 1: HR = 1.447, 95% CI 1.255-1.669, P < 0.001; Model 2: HR = 1.252, 95% CI 1.045-1.499, P = 0.015; Model 3: HR = 1.284, 95% CI 1.071-1.539, P = 0.007). Subgroup stratified analyses showed that AIP might interact with sex, a classical risk factor of cardiovascular events.
This study showed that AIP might be a strong biomarker that could be used to predict the risk of cardiovascular events in patients with T2DM.
URL: http://www.clinicaltrials.gov . Unique identifier: NCT00000620.
先前的研究报告了血浆致动脉粥样硬化指数(AIP)在动脉粥样硬化和其他心血管疾病(CVDs)病程中的预后价值。然而,AIP 在 2 型糖尿病(T2DM)患者中的预测效用尚不清楚。
这是对“行动控制心血管风险在糖尿病(ACCORD)研究”的二次分析,该研究随机分配了 10251 名长期 T2DM 患者。使用 ROC 曲线分析确定 AIP 的最佳阈值,并将研究人群分为高 AIP 组和低 AIP 组。使用单变量和多变量 Cox 比例风险回归分析来确定 AIP 与主要(主要不良心血管事件[MACE],包括非致死性心肌梗死、非致死性卒中和/或心血管原因死亡)和次要结局(全因死亡率)之间的关联。进行分层分析以控制混杂因素。
AIP 是 T2DM 预后的独立危险因素(HR=1.309;95%CI 1.084-1.581;P=0.005)。研究人群中确定 AIP 的阈值为 0.34。在调整混杂因素后,多变量分析表明 AIP 与 MACE 的风险相关(模型 1:HR=1.333,95%CI 1.205-1.474,P<0.001;模型 2:HR=1.171,95%CI 1.030-1.333,P=0.016;模型 3:HR=1.194,95%CI 1.049-1.360,P=0.007),全因死亡率(模型 1:HR=1.184,95%CI 1.077-1.303,P<0.001),心血管死亡(模型 1:HR=1.422,95%CI 1.201-1.683,P<0.001;模型 3:HR=1.264,95%CI 1.015-1.573,P=0.036),非致死性心肌梗死(模型 1:HR=1.447,95%CI 1.255-1.669,P<0.001;模型 2:HR=1.252,95%CI 1.045-1.499,P=0.015;模型 3:HR=1.284,95%CI 1.071-1.539,P=0.007)。分层亚组分析表明,AIP 可能与心血管事件的经典危险因素性别存在交互作用。
本研究表明,AIP 可能是一种强大的生物标志物,可用于预测 T2DM 患者心血管事件的风险。