Myers Risa B, Ruiz Joseph R, Jermaine Christopher M, Nates Joseph L
Department of Computer Science, Rice University, Texas, USA.
Children's Environmental Health Initiative, Rice University, Texas, USA.
J Surg Oncol (Tallinn). 2020;3. doi: 10.31487/j.jso.2020.01.10. Epub 2020 Mar 10.
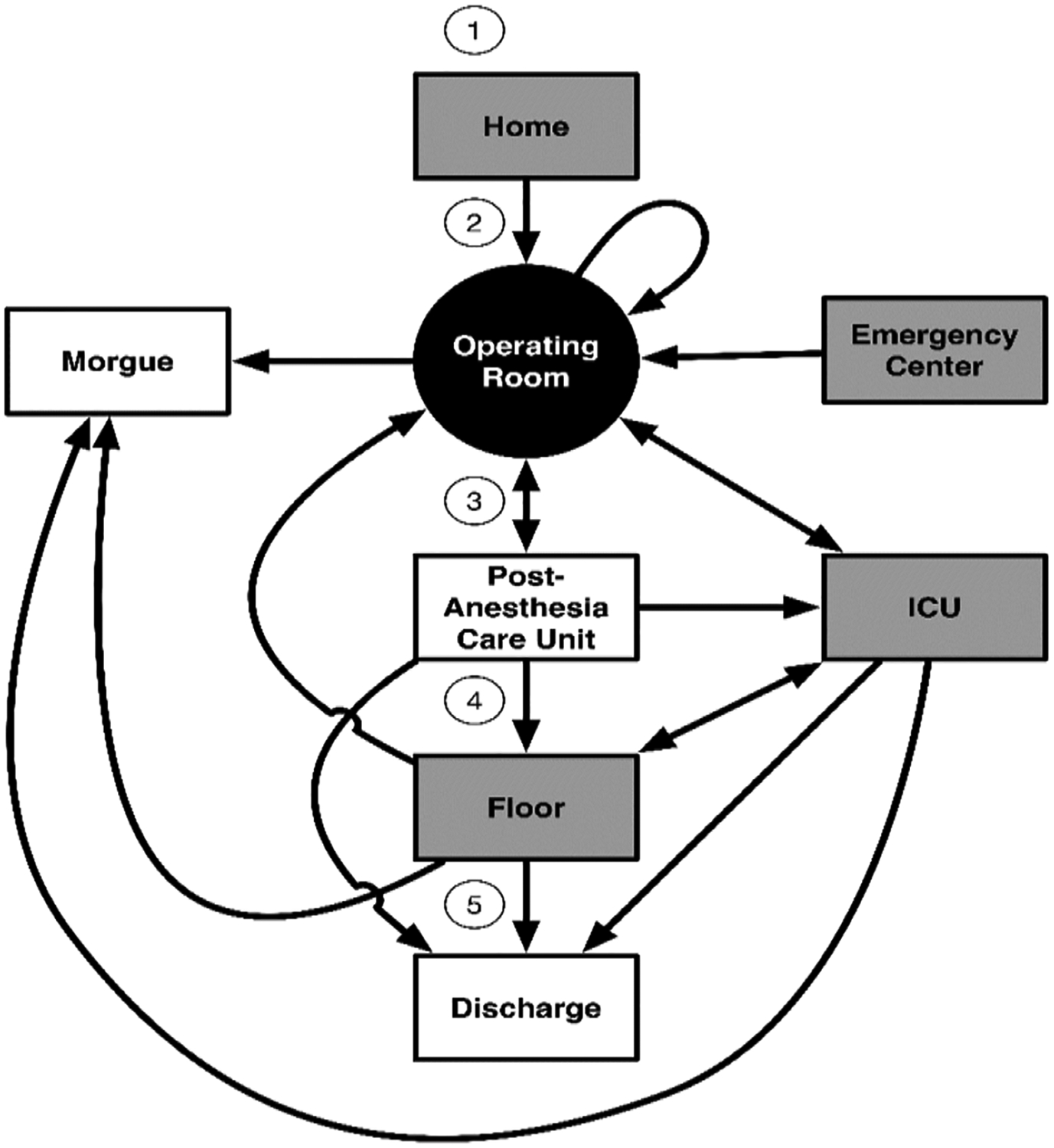
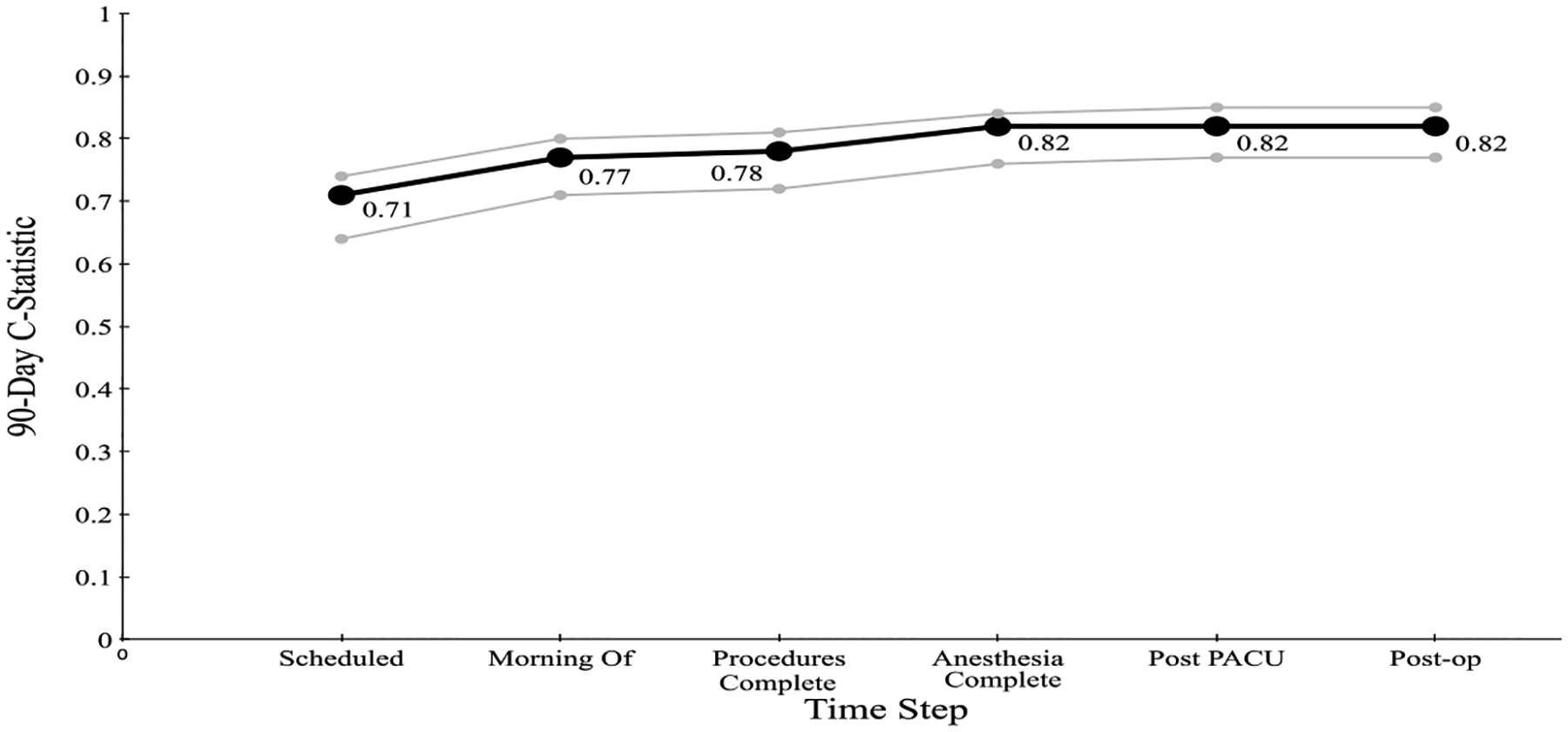
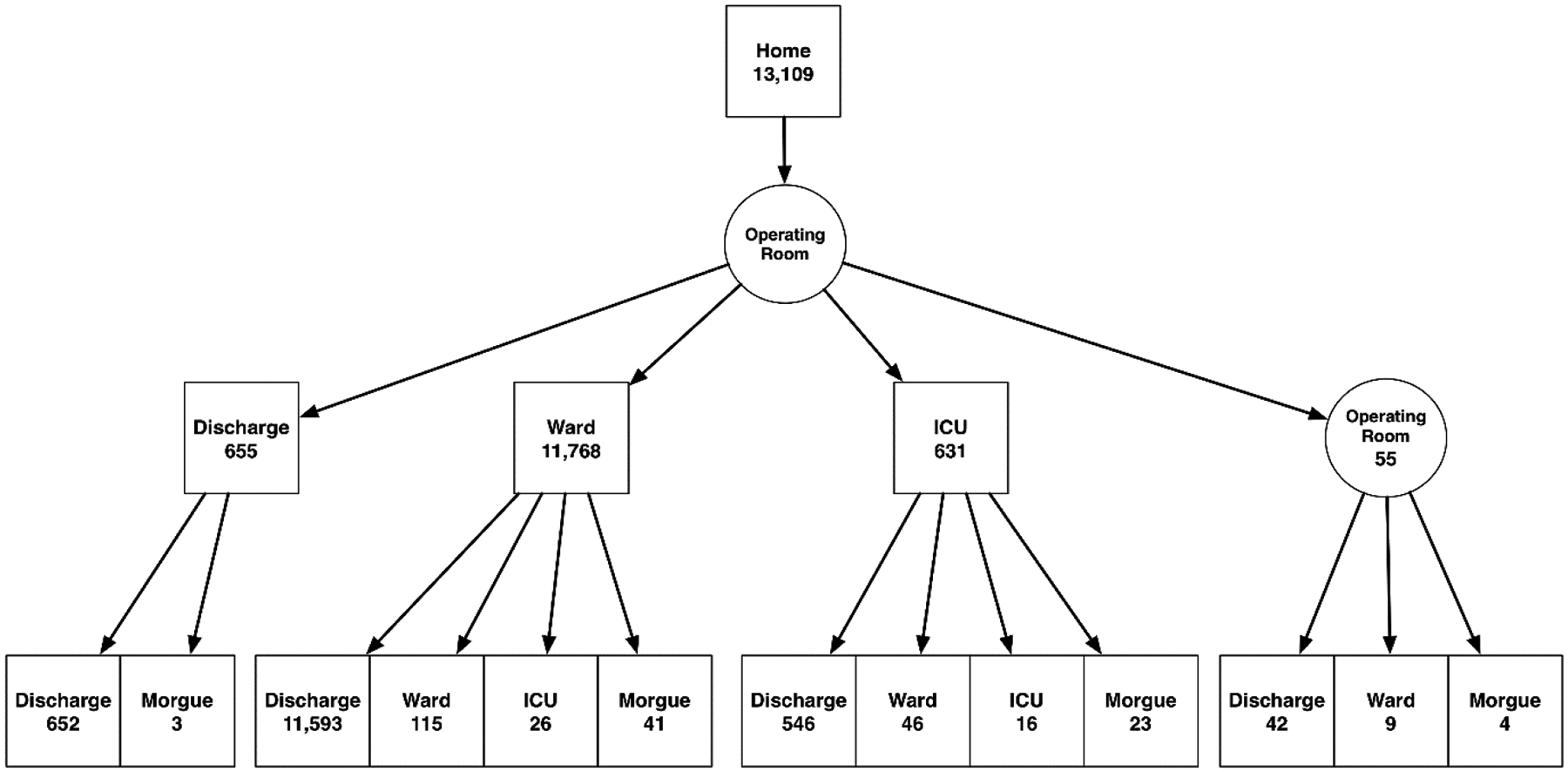
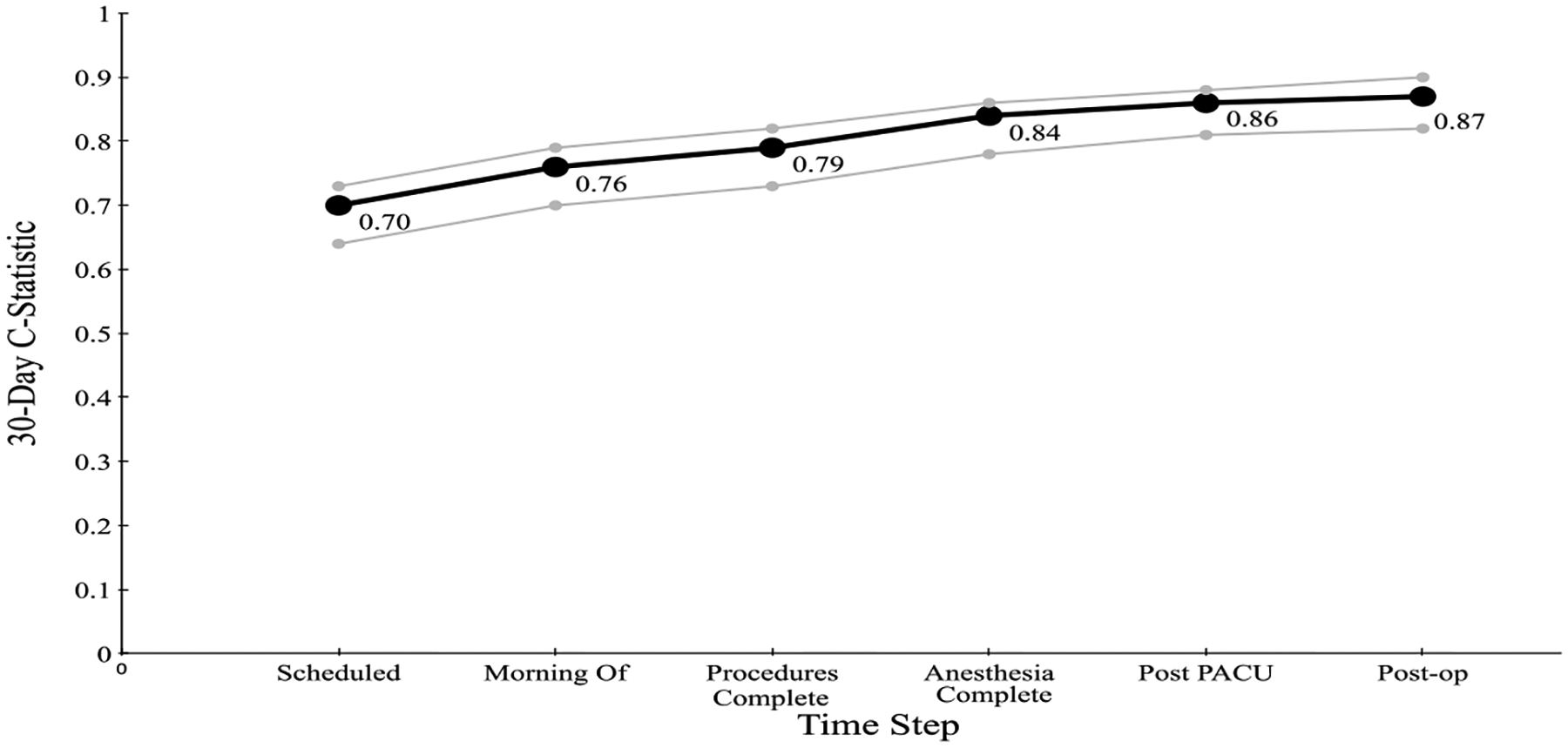
We constructed a multivariate logistic regression model of 30 (90)-day mortality, which occurred in 106 (290) of the cases, using 13,877 major abdominal surgical cases performed at the University of Texas MD Anderson Cancer Center from January 2007 to March 2014. The model includes race, starting location (home, inpatient ward, intensive care unit or emergency center), Charlson Comorbidity Index, emergency status, ASA-PS classification, procedure, surgical Apgar score, destination after surgery (hospital ward location) and delayed intensive care unit admit within six days. We computed and compared the model mortality prediction ability (C-statistic) as we accumulated features over time.
We were able to predict 30 (90)-day mortality with C-statistics from 0.70 (0.71) initially to 0.87 (0.84) within six days postoperatively.
We achieved a high level of model discrimination. The CPM enables a continuous cumulative assessment of the patient's mortality risk, which could then be used as a decision support aid regarding patient care and treatment, potentially resulting in improved outcomes, decreased costs and more informed decisions.
1)利用腹部外科癌症患者的医院临床病程建立一个累积围手术期模型(CPM),以预测30天和90天的死亡风险;2)将该模型的预测能力与其他十个现有模型进行比较。
我们使用2007年1月至2014年3月在德克萨斯大学MD安德森癌症中心进行的13877例主要腹部外科手术病例,构建了一个30(90)天死亡率的多因素逻辑回归模型,其中106(290)例出现了30(90)天死亡。该模型包括种族、起始地点(家中、住院病房、重症监护病房或急诊中心)、查尔森合并症指数、急诊状态、美国麻醉医师协会身体状况分级(ASA-PS)、手术、手术阿普加评分、术后目的地(医院病房位置)以及术后六天内延迟入住重症监护病房的情况。随着时间的推移,我们在积累特征的过程中计算并比较了模型的死亡率预测能力(C统计量)。
我们能够预测30(90)天死亡率,术后六天内C统计量从最初的0.70(0.71)提高到0.87(0.84)。
我们实现了较高水平的模型区分度。CPM能够对患者的死亡风险进行连续的累积评估,进而可作为患者护理和治疗的决策支持工具,有可能改善治疗结果、降低成本并做出更明智的决策。