Dyson Greg
Department of Oncology, Karmanos Cancer Institute, Wayne State University, Detroit MI, USA.
Int J Clin Biostat Biom. 2021;7(1). doi: 10.23937/2469-5831/1510038. Epub 2021 Jun 28.
Phase III superiority clinical trials have negative results (new treatment is not statistically better than standard of care) due to a number of factors, including patient and disease heterogeneity. However, even a treatment regime that fails to show population-level clinical improvement will have a subgroup of patients that attain a measurable clinical benefit.
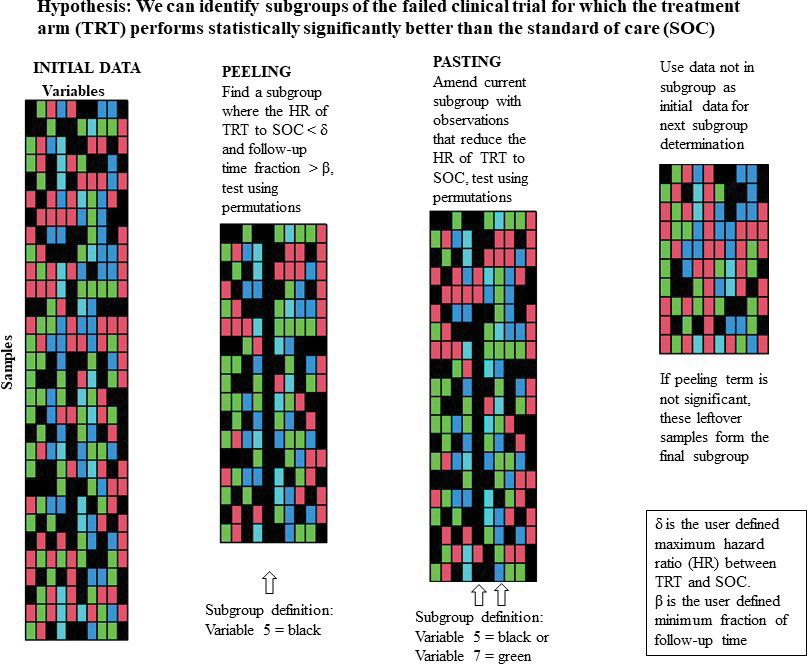
The goal of this paper is to modify the Patient Rule-Induction Method to identify statistically significant subgroups, defined by clinical and/or demographic factors, of the clinical trial population where the experimental treatment performs better than the standard of care and better than observed in the entire clinical trial sample.
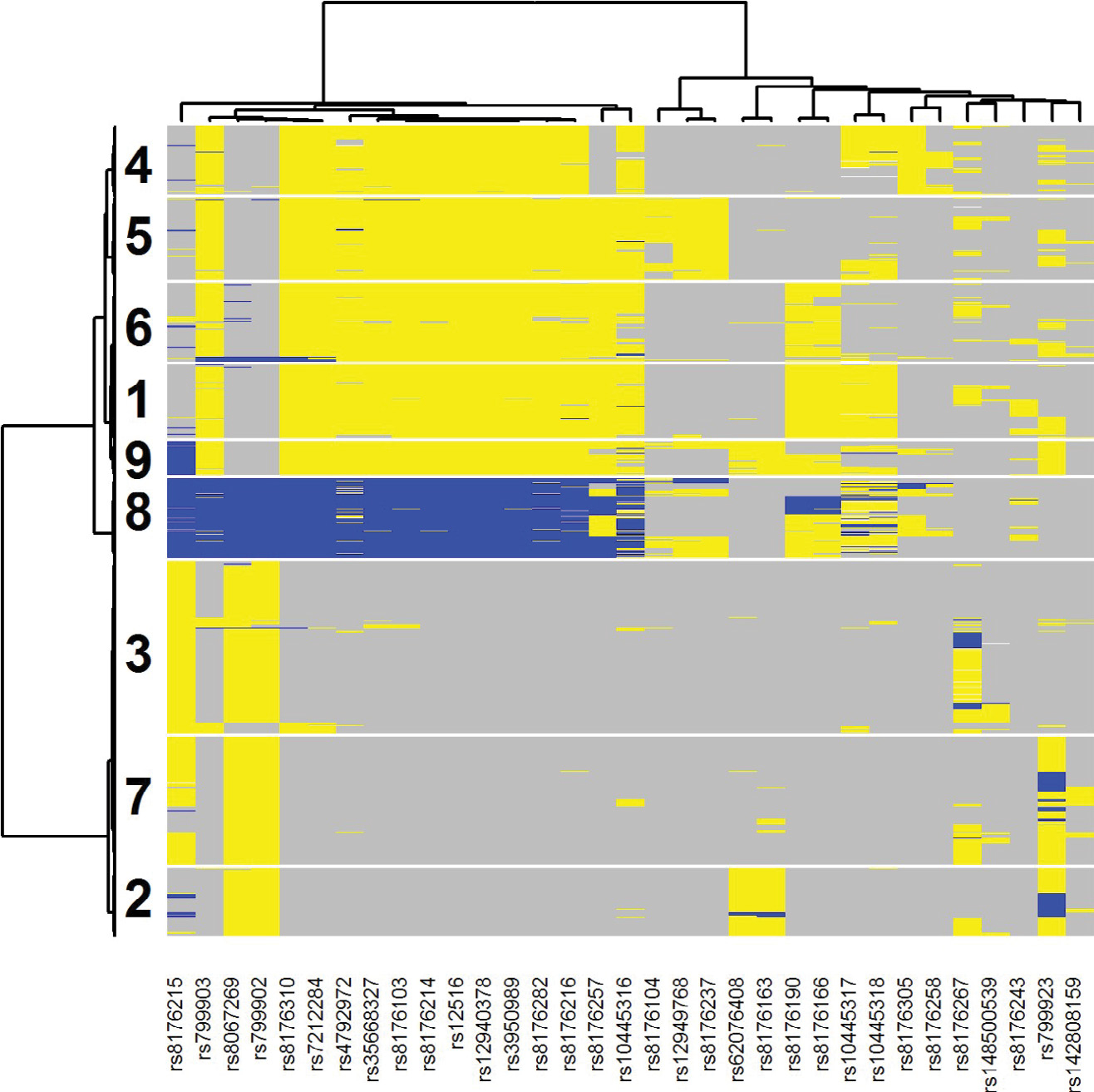
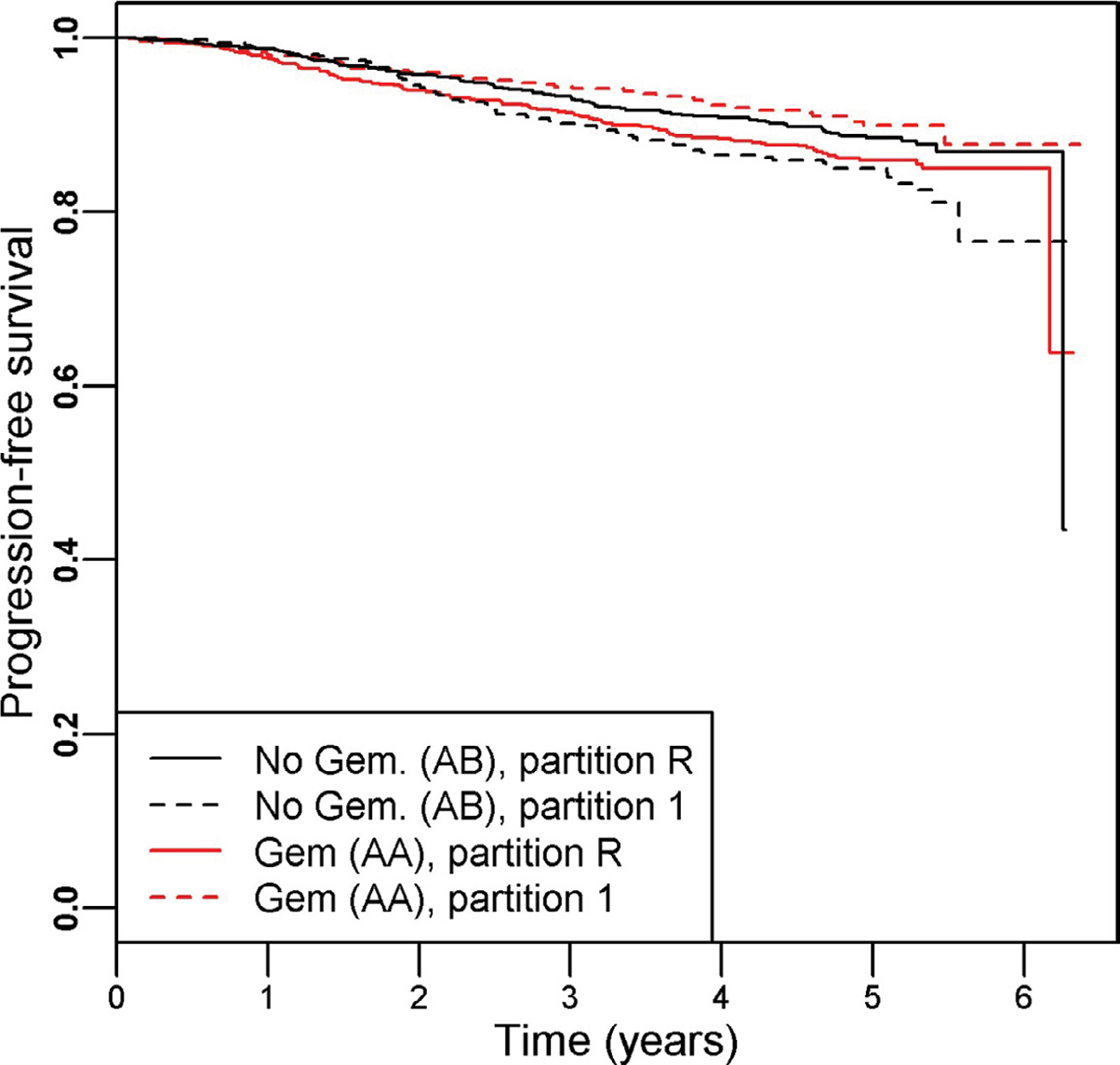
We illustrate this method using part A of the SUCCESS clinical trial, which showed no overall difference between treatment arms: HR (95% CI) = 0.97 (0.78, 1.20). Using PRIM, we identified one subgroup defined by the mutational profile in BRCA1 which resulted in a significant benefit for adding Gemcitabine to the standard treatment: HR (95% CI) = 0.59 (0.40, 0.87).
This result demonstrates that useful information can be extracted from existing databases that could provide insight into why a phase III trial failed and assist in the design of future clinical trials involving the experimental treatment.
由于包括患者和疾病异质性在内的多种因素,III期优效性临床试验会得出阴性结果(新疗法在统计学上并不优于标准治疗)。然而,即使一种治疗方案未能显示出总体临床改善,也会有一部分患者获得可测量的临床益处。
本文的目的是修改患者规则归纳法,以识别由临床和/或人口统计学因素定义的具有统计学意义的亚组,在该亚组中,试验性治疗比标准治疗表现更好,且优于在整个临床试验样本中观察到的情况。
我们使用SUCCESS临床试验的A部分来说明这种方法,该部分显示各治疗组之间没有总体差异:风险比(95%置信区间)=0.97(0.78,1.20)。使用PRIM,我们确定了一个由BRCA1突变谱定义的亚组,该亚组显示在标准治疗中添加吉西他滨有显著益处:风险比(95%置信区间)=0.59(0.40,0.87)。
这一结果表明,可以从现有数据库中提取有用信息,这些信息可以深入了解III期试验失败的原因,并有助于设计未来涉及试验性治疗的临床试验。