College of Medicine and Health, University of Exeter, Exeter, UK.
Deep Dementia Phenotyping (DEMON) Network, Exeter, UK.
Alzheimers Res Ther. 2021 Oct 11;13(1):169. doi: 10.1186/s13195-021-00895-4.
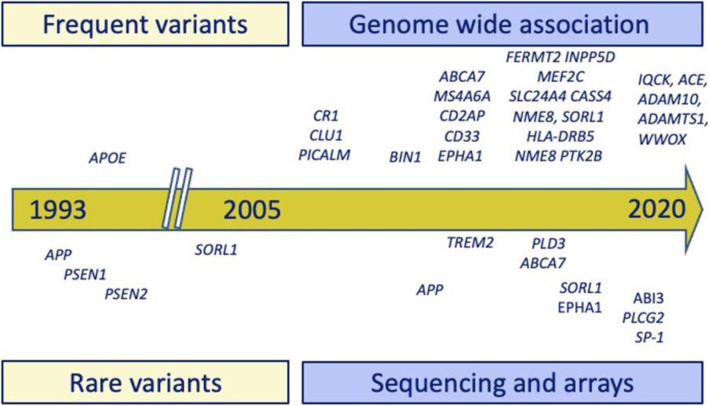
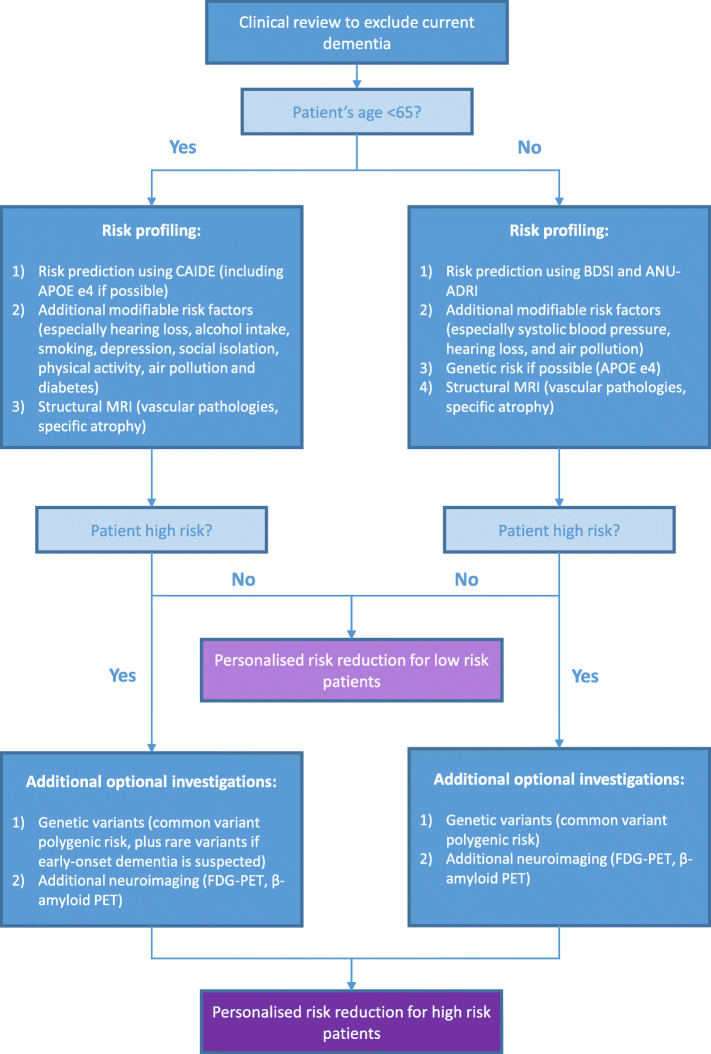
We envisage the development of new Brain Health Services to achieve primary and secondary dementia prevention. These services will complement existing memory clinics by targeting cognitively unimpaired individuals, where the focus is on risk profiling and personalized risk reduction interventions rather than diagnosing and treating late-stage disease. In this article, we review key potentially modifiable risk factors and genetic risk factors and discuss assessment of risk factors as well as additional fluid and imaging biomarkers that may enhance risk profiling. We then outline multidomain measures and risk profiling and provide practical guidelines for Brain Health Services, with consideration of outstanding uncertainties and challenges. Users of Brain Health Services should undergo risk profiling tailored to their age, level of risk, and availability of local resources. Initial risk assessment should incorporate a multidomain risk profiling measure. For users aged 39-64, we recommend the Cardiovascular Risk Factors, Aging, and Incidence of Dementia (CAIDE) Dementia Risk Score, whereas for users aged 65 and older, we recommend the Brief Dementia Screening Indicator (BDSI) and the Australian National University Alzheimer's Disease Risk Index (ANU-ADRI). The initial assessment should also include potentially modifiable risk factors including sociodemographic, lifestyle, and health factors. If resources allow, apolipoprotein E ɛ4 status testing and structural magnetic resonance imaging should be conducted. If this initial assessment indicates a low dementia risk, then low intensity interventions can be implemented. If the user has a high dementia risk, additional investigations should be considered if local resources allow. Common variant polygenic risk of late-onset AD can be tested in middle-aged or older adults. Rare variants should only be investigated in users with a family history of early-onset dementia in a first degree relative. Advanced imaging with 18-fluorodeoxyglucose positron emission tomography (FDG-PET) or amyloid PET may be informative in high risk users to clarify the nature and burden of their underlying pathologies. Cerebrospinal fluid biomarkers are not recommended for this setting, and blood-based biomarkers need further validation before clinical use. As new technologies become available, advances in artificial intelligence are likely to improve our ability to combine diverse data to further enhance risk profiling. Ultimately, Brain Health Services have the potential to reduce the future burden of dementia through risk profiling, risk communication, personalized risk reduction, and cognitive enhancement interventions.
我们设想开发新的大脑健康服务,以实现初级和二级痴呆预防。这些服务将通过针对认知未受损个体来补充现有的记忆诊所,重点是风险分析和个性化的风险降低干预,而不是诊断和治疗晚期疾病。在本文中,我们回顾了关键的潜在可改变的风险因素和遗传风险因素,并讨论了风险因素的评估以及可能增强风险分析的其他液体和成像生物标志物。然后,我们概述了多领域措施和风险分析,并为大脑健康服务提供了实用的指南,同时考虑了未解决的不确定性和挑战。大脑健康服务的使用者应根据其年龄、风险水平和当地资源的可用性进行量身定制的风险分析。初始风险评估应包括多领域风险分析措施。对于 39-64 岁的使用者,我们建议使用心血管风险因素、衰老和痴呆发生率(CAIDE)痴呆风险评分;而对于 65 岁及以上的使用者,我们建议使用简短的痴呆筛查指标(BDSI)和澳大利亚国立大学阿尔茨海默病风险指数(ANU-ADRI)。初始评估还应包括潜在的可改变的风险因素,包括社会人口统计学、生活方式和健康因素。如果资源允许,应进行载脂蛋白 E ɛ4 状态检测和结构磁共振成像。如果初始评估表明痴呆风险较低,则可以实施低强度干预措施。如果使用者痴呆风险较高,并且当地资源允许,应考虑进行额外的调查。常见变异多基因晚发性 AD 风险可以在中年或老年人中进行检测。只有在一级亲属中有早发性痴呆家族史的使用者中,才应调查罕见变异。在高危使用者中,使用 18-氟脱氧葡萄糖正电子发射断层扫描(FDG-PET)或淀粉样蛋白 PET 进行高级成像可能有助于阐明其潜在病理的性质和负担。不建议在此环境下使用脑脊液生物标志物,血液生物标志物在临床使用前需要进一步验证。随着新技术的出现,人工智能的进步可能会提高我们结合多种数据以进一步增强风险分析的能力。最终,大脑健康服务通过风险分析、风险沟通、个性化风险降低和认知增强干预,有可能降低未来痴呆的负担。