Kidney Center, Turku University Hospital and University of Turku, Building 4, AA7, Kiinanmyllynkatu 4-8, FIN-20521 Turku, Finland.
Department of Anaesthesiology and Intensive Care, Turku University Hospital and University of Turku, Building 18, TG3B, Hämeentie 11, FIN-20521 Turku, Finland.
Int J Mol Sci. 2021 Sep 23;22(19):10238. doi: 10.3390/ijms221910238.
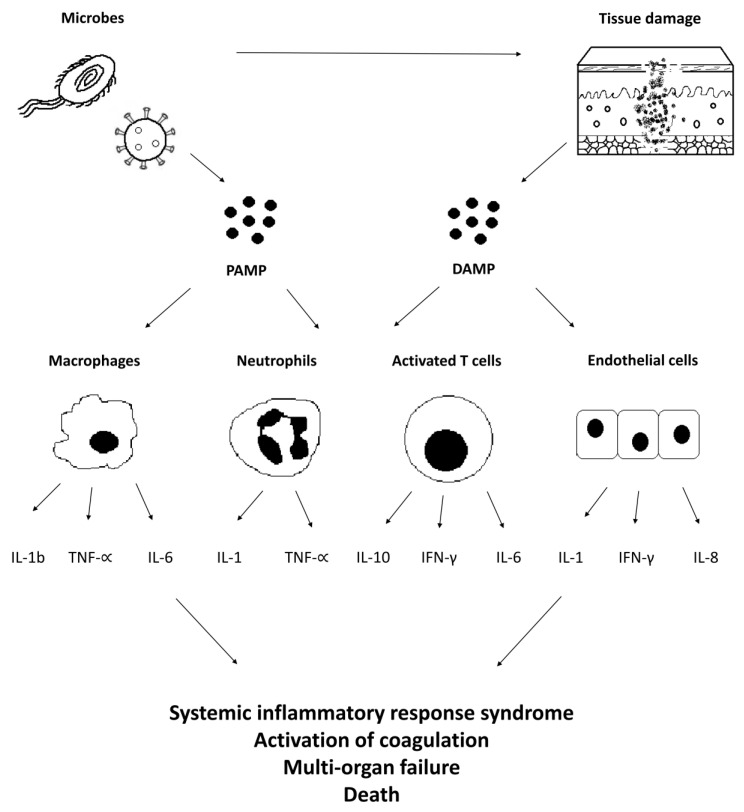
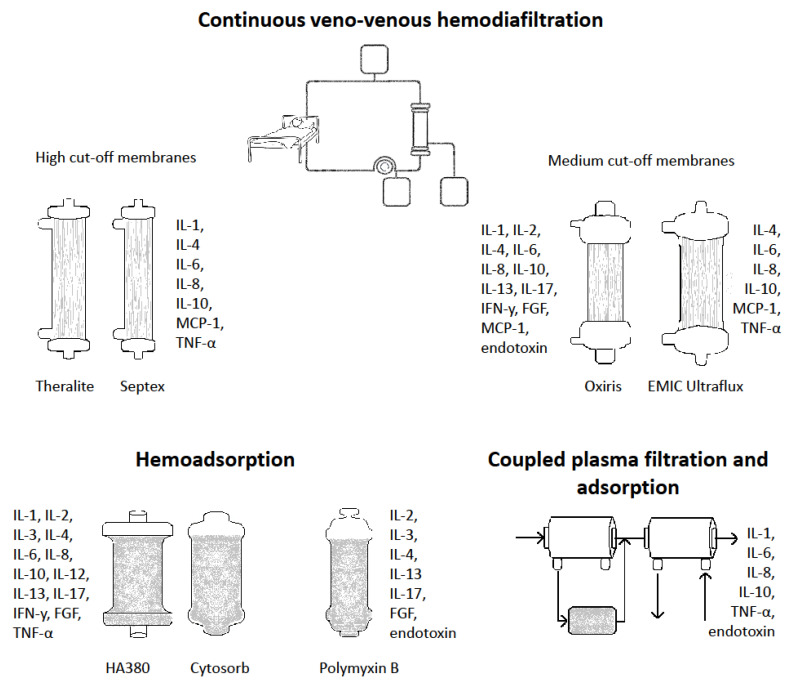
Sepsis is defined as a life-threatening organ dysfunction caused by a dysregulated host response to an infection; it carries a risk for mortality, considerably exceeding that of a mere infection. Sepsis is the leading cause for acute kidney injury (AKI) and the requirement for renal replacement therapy (RRT) in intensive care unit (ICU) patients. Almost every second critically ill patient with sepsis will develop AKI. In septic shock, the dysregulated host response to infectious pathogens leads to a cytokine storm with uncontrolled production and release of humoral proinflammatory mediators that evoke cellular toxicity and promote the development of organ dysfunction and increased mortality. In addition to treating AKI, RRT techniques can be employed for extracorporeal adsorption of inflammatory mediators using specifically developed adsorption membranes, hemoperfusion sorbent cartridges or columns; these techniques are intended to decrease the level and early deleterious effects of circulating proinflammatory cytokines and endotoxins during the first hours and days of septic shock treatment, in order to improve patient outcomes. Several methods and devices, such as high cut-off membranes, the Oxiris-AN69 membrane, CytoSorb and HA380 cytokine hemoadsorption, polymyxin B endotoxin adsorption, and plasmapheresis have been examined in small study series or are under evaluation as ways of improving patient outcomes in septic shock. However, to date, the data on actual outcome benefits have remained controversial, as discussed in this review.
脓毒症是一种由宿主对感染的失调反应引起的危及生命的器官功能障碍;它的死亡率风险非常高,远远超过单纯的感染。脓毒症是重症监护病房(ICU)患者急性肾损伤(AKI)和肾脏替代治疗(RRT)的主要原因。几乎每两个患有脓毒症的危重症患者中就有一个会发生 AKI。在感染性休克中,宿主对感染病原体的失调反应会导致细胞毒性细胞因子风暴,失控地产生和释放体液促炎介质,促进器官功能障碍和死亡率增加。除了治疗 AKI 外,RRT 技术还可用于使用专门开发的吸附膜、血液灌流吸附剂盒或柱体外吸附炎症介质;这些技术旨在降低感染性休克治疗最初几小时和几天内循环促炎细胞因子和内毒素的水平和早期有害作用,以改善患者预后。已经在小型研究系列中检查了几种方法和设备,如高截止膜、Oxiris-AN69 膜、CytoSorb 和 HA380 细胞因子血液吸附、多粘菌素 B 内毒素吸附和血浆置换,作为改善感染性休克患者预后的方法正在评估中。然而,到目前为止,关于实际结果获益的数据仍然存在争议,正如本文综述所讨论的那样。