Kidney Center, Turku University Hospital and University of Turku, Turku, Finland.
Department of Anaesthesiology and Intensive Care, University of Turku, Turku, Finland.
PLoS One. 2021 Apr 5;16(4):e0249561. doi: 10.1371/journal.pone.0249561. eCollection 2021.
Septic acute kidney injury (AKI) requiring continuous renal replacement therapy (CRRT) carries a mortality risk nearing 50%. Risk factors associated with mortality in AKI patients undergoing CRRT with blood culture positive sepsis remain unclear as sepsis has been defined according to consensus criteria in previous studies.
Risk factors associated with intensive care unit (ICU), 90-day and overall mortality were studied in a retrospective cohort of 126 patients with blood culture positive sepsis and coincident severe AKI requiring CRRT. Comprehensive laboratory and clinical data were gathered at ICU admission and CRRT initiation.
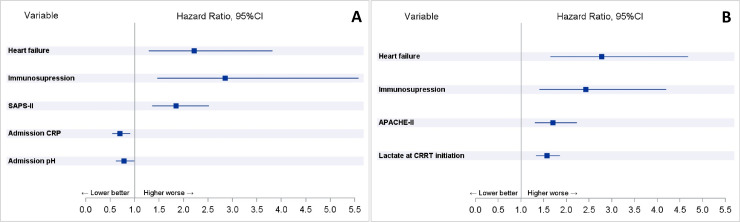
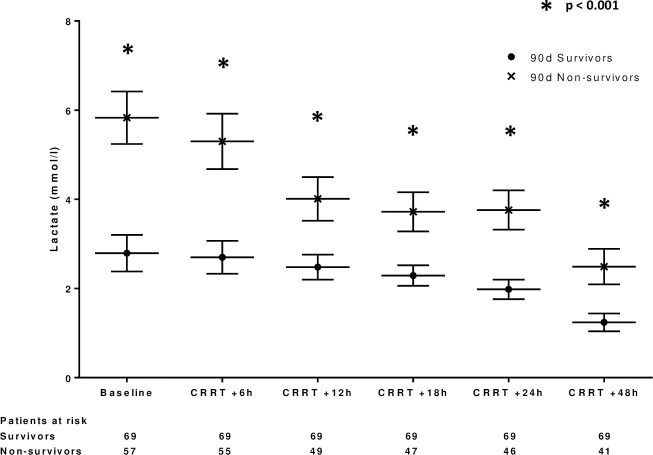
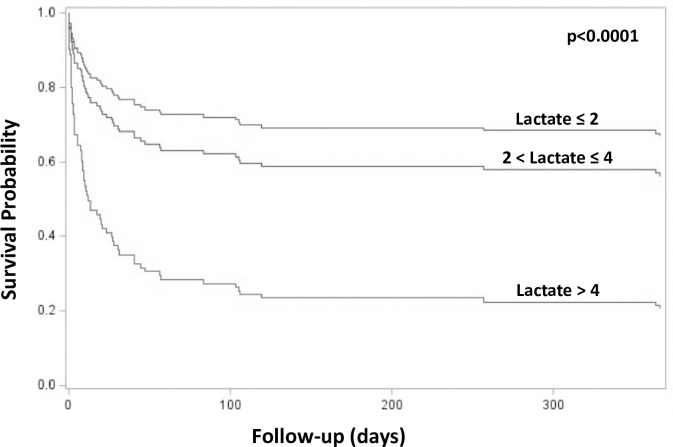
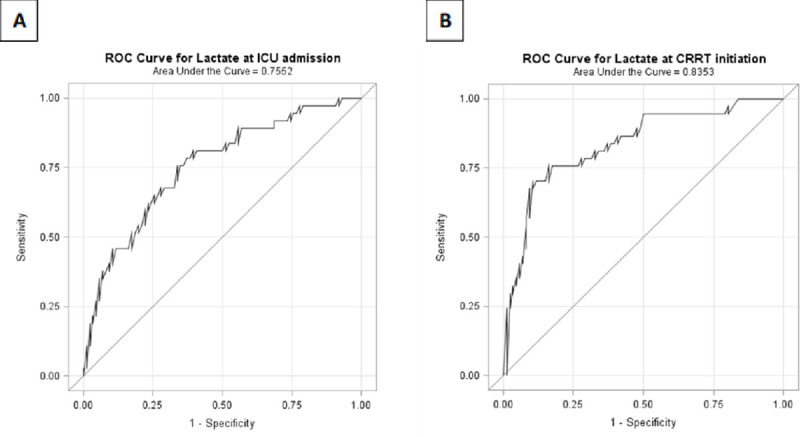
38 different causative pathogens for sepsis and associated AKI were identified. ICU mortality was 30%, 90-day mortality 45% and one-year mortality 50%. Immunosuppression, history of heart failure, APACHE II and SAPS II scores, C-reactive protein and lactate at CRRT initiation were independently associated with mortality in multivariable Cox proportional hazards models. Blood lactate showed good predictive power for ICU mortality in receiver operating characteristic curve analyses with AUCs of 0.76 (95%CI 0.66-0.85) for lactate at ICU admission and 0.84 (95%CI 0.72-0.95) at CRRT initiation.
Our study shows for the first time that lactate measured at CRRT initiation is predictive of ICU mortality and independently associated with overall mortality in patients with blood culture positive sepsis and AKI requiring CRRT. Microbial etiology for septic AKI requiring CRRT is diverse.
需要连续性肾脏替代治疗(CRRT)的脓毒症急性肾损伤(AKI)死亡率接近 50%。在接受血培养阳性脓毒症并同时发生严重 AKI 需要 CRRT 的 AKI 患者中,与死亡率相关的危险因素仍不清楚,因为在以前的研究中,脓毒症是根据共识标准定义的。
对 126 例血培养阳性脓毒症合并严重 AKI 需要 CRRT 的患者进行回顾性队列研究,分析与 ICU、90 天和总死亡率相关的危险因素。在 ICU 入院和 CRRT 开始时收集全面的实验室和临床数据。
确定了 38 种不同的导致脓毒症和相关 AKI 的病原体。ICU 死亡率为 30%,90 天死亡率为 45%,1 年死亡率为 50%。免疫抑制、心力衰竭史、APACHE II 和 SAPS II 评分、CRRT 开始时的 C 反应蛋白和乳酸与多变量 Cox 比例风险模型中的死亡率独立相关。在接受者操作特征曲线分析中,血乳酸在 ICU 入院时的 AUC 为 0.76(95%CI 0.66-0.85),在 CRRT 开始时的 AUC 为 0.84(95%CI 0.72-0.95),表明乳酸对 ICU 死亡率具有良好的预测能力。
我们的研究首次表明,CRRT 开始时测量的乳酸可预测 ICU 死亡率,并与需要 CRRT 的血培养阳性脓毒症和 AKI 患者的总死亡率独立相关。需要 CRRT 的脓毒症性 AKI 的微生物病因多种多样。