Troppmair Teresa, Egger J, Krösbacher A, Zanvettor A, Schinnerl A, Neumayr A, Baubin M
Universitätsklinik für Anästhesie und Intensivmedizin, Anichstraße 35, 6020, Innsbruck, Österreich.
Anaesthesist. 2022 Apr;71(4):272-280. doi: 10.1007/s00101-021-01046-y. Epub 2021 Oct 13.
Human and vehicle resource management indicates a good emergency medical system (EMS). Frequently, an emergency medical technician (EMT) is the first responder to the emergency, which negates the necessity for an emergency physician (EP) and is just as sensible as handing over a stable patient to the EMT for transport to the hospital. The Austrian EMS is utilized by EMTs, in cases of potential life-threatening emergencies the dispatch center dispatches an additional team with an on-board EP. During the years 2017-2018 nearly every fifth EP mission in Innsbruck (including surrounding areas) ended in a cancellation. The numbers of patient handovers from EP to EMT are slightly lower with mission cancellations resulting in every fourth patient. Therefore, due to the high number of cancellations and handovers evaluated in this study, the findings suggest that there is a potential need to re-evaluate procedures. The re-evaluation of these procedures could determine whether these cancellations/handovers were justified or if an over hasty decision making was at fault. All cases considered in this study were from the Innsbruck and Telfs EP bases between 1 January 2017 and 13 December 2018.
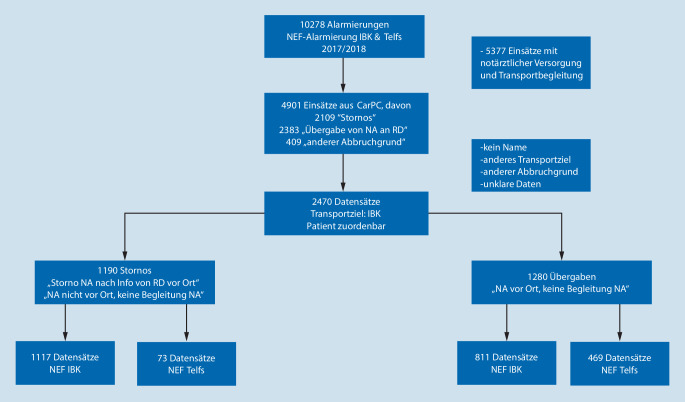
Out of a total of 96,908 emergency dispatches, there were 2470 cancellation/handover occurrences. These occurrences consisted of 1190 cancellations and 1280 patient handovers from the EP to the EMT. Patients who were transferred to the University Hospital Innsbruck were included in these figures. The protocols of the emergency dispatches have been filtered from the so-called CarPC. They have subsequently been grouped into cancellation and handover categories. The clinical diagnoses of the patients with inpatient treatment were evaluated from the hospital information system (KIS) of the University Hospital Innsbruck. This was done with the help of the so-called emergency physician indications catalogue of the German Medical Council. The diagnosis was documented in the hospital information system. The emergency protocols from the EMTs were also evaluated retrospectively. The Innsbruck based EP patients are hospitalized in the Innsbruck Hospital due their geographical position. When there is no need for a specific intervention the patients of the EPs based in Telfs are transferred to a local hospital. When a specific intervention is necessary, patient care must be provided by the University Hospital Innsbruck. Due to the privacy practices of the Innsbruck Medical University "vote of ethics" only the data of patients transferred to the Innsbruck Clinic can be evaluated. The information provided from the EPs based in Innsbruck was exclusively from the University Hospital Innsbruck's anesthesiologists. The physicians from the Telfs EP base are of mixed medical specialities. All of them, however, have an emergency medical physician diploma, in addition to the ius practicandi. Lastly, there are no EPs in Innsbruck or Telfs, who have any special obligations during their duty.
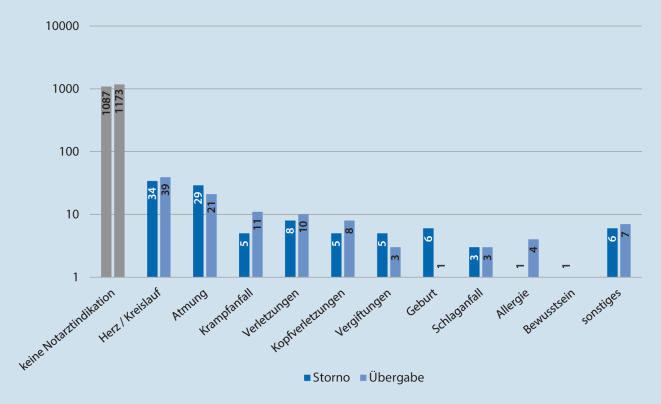
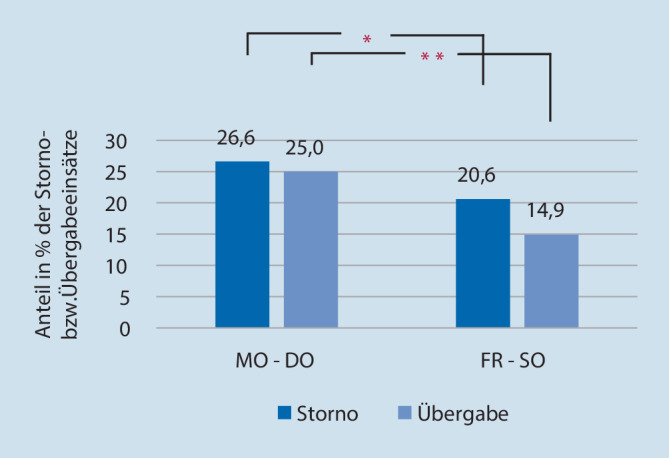
The results show that in 210 cases (8.5%) the indications for the EP, based on the emergency physician indications catalogue of the German Medical Council were given. Also, 8.7% of all cancellations and 8.4% of patient handovers were not justified. Patients with emergency indications had a longer hospitalization. The EP base EMS Innsbruck had more cancellations than the EP base EMS Telfs. The EMS Innsbruck also had more cancellations than patient handovers. Conversely, the EMS Telfs had more patient handovers than cancellations. On the weekends between 6:00 pm and 6:00 am there were less cancellations and handovers from both EP bases. The documentation from the EMT protocols was incomplete in 284 cancellations (23.9% of the cancellations) and 339 handovers (26.5% of the handovers), 35 patients after cancellations (2.9%), 35 patients after handovers (2.7%) needed intensive care treatment, 20 patients after cancellations (1.7% of all cancellations), and 24 patients after handovers (1.9% of all handovers) who needed intensive care treatment had a critical diagnosis. In 40 cases of patient handovers, the EP was alerted to another emergency follow-up within 10 min.
In Austria, the introduction of a standardized emergency indication checklist might help dispatch centers to provide a more accurate dispatch as well as all EMS team members. Furthermore, a better traceability system (according to EP cancellations and patient handovers from the EP to the EMT) could be achieved. The documentation requirements should be more precise by all members of the EMT staff, not only for the legal aspects but also for improving the overall management quality. Intense education and training as well as diagnosis feedbacks could help to reduce the number of risky cancellations/patient handovers.
人力和车辆资源管理体现了良好的紧急医疗系统(EMS)。通常,急救医疗技术员(EMT)是紧急情况的第一响应者,这使得急诊医生(EP)并非必需,就如同将病情稳定的患者交给EMT送往医院一样合理。奥地利的EMS由EMT使用,在潜在危及生命的紧急情况下,调度中心会派遣一个额外配备随车EP的团队。在2017 - 2018年期间,因斯布鲁克(包括周边地区)几乎每五次EP任务中就有一次以取消告终。从EP向EMT的患者交接数量略低,每四次患者交接中就有一次任务取消。因此,鉴于本研究中评估的取消和交接数量众多,研究结果表明可能需要重新评估程序。对这些程序的重新评估可以确定这些取消/交接是否合理,或者是否存在决策过于仓促的问题。本研究考虑的所有病例均来自2*017年1月1日至2018年12月13日期间因斯布鲁克和特尔夫斯的EP基地。
在总共96908次紧急调度中,有2470次取消/交接事件。这些事件包括1190次取消和1280次从EP到EMT的患者交接。转至因斯布鲁克大学医院的患者包括在这些数据中。紧急调度的协议已从所谓的CarPC中筛选出来。随后它们被分为取消和交接类别。住院治疗患者的临床诊断是从因斯布鲁克大学医院的医院信息系统(KIS)中评估的。这是借助德国医学委员会所谓的急诊医生指征目录完成的。诊断记录在医院信息系统中。EMT的紧急协议也进行了回顾性评估。因斯布鲁克基地的EP患者因其地理位置在因斯布鲁克医院住院。当不需要特定干预时,特尔夫斯基地的EP患者被转至当地医院。当需要特定干预时,必须由因斯布鲁克大学医院提供患者护理。由于因斯布鲁克医科大学的隐私规定,“伦理投票”仅可评估转至因斯布鲁克诊所的患者数据。因斯布鲁克基地的EP提供的信息仅来自因斯布鲁克大学医院的麻醉医生。特尔夫斯EP基地的医生具有多种医学专业。然而,他们所有人除了行医资格外,都拥有急诊医生文凭。最后,因斯布鲁克或特尔夫斯没有EP在值班期间有任何特殊义务。
结果显示,根据德国医学委员会的急诊医生指征目录,在210例(8.5%)病例中给出了EP的指征。此外,所有取消事件中的8.7%和患者交接事件中的8.4%不合理。有紧急指征的患者住院时间更长。因斯布鲁克基地的EMS取消事件比特尔夫斯基地的EMS多。因斯布鲁克的EMS取消事件也比患者交接事件多。相反,特尔夫斯的EMS患者交接事件比取消事件多。在周末下午6:00至上午6:00之间,两个EP基地的取消和交接事件较少。EMT协议的记录在284次取消事件(占取消事件的23.9%)和339次交接事件(占交接事件的26.5%)中不完整,取消事件后有35名患者(2.9%)、交接事件后有35名患者(2.7%)需要重症监护治疗,取消事件后有20名患者(占所有取消事件的1.7%)、交接事件后有24名患者(占所有交接事件的1.9%)需要重症监护治疗且诊断危急。在40例患者交接事件中,EP在10分钟内接到了另一个紧急后续通知。
在奥地利,引入标准化的紧急指征清单可能有助于调度中心以及所有EMS团队成员进行更准确的调度。此外,可以实现更好的可追溯系统(根据EP取消事件以及从EP到EMT的患者交接)。EMT工作人员的所有成员都应使文件记录要求更加精确,这不仅是出于法律方面的考虑,也是为了提高整体管理质量。强化教育和培训以及诊断反馈有助于减少有风险的取消/患者交接数量。