Department of General Practice, Amsterdam University Medical Center, Vrije Universiteit, Amsterdam, The Netherlands.
Department of Epidemiology and Data Science, Amsterdam University Medical Center, Vrije Universiteit, Amsterdam, The Netherlands.
BMC Geriatr. 2021 Oct 14;21(1):551. doi: 10.1186/s12877-021-02521-2.
Accurate identification of older persons at risk of unplanned hospital visits can facilitate preventive interventions. Several risk scores have been developed to identify older adults at risk of unplanned hospital visits. It is unclear whether risk scores developed in one country, perform as well in another. This study validates seven risk scores to predict unplanned hospital admissions and emergency department (ED) visits in older home care recipients from six countries.
We used the IBenC sample (n = 2446), a cohort of older home care recipients from six countries (Belgium, Finland, Germany, Iceland, Italy and The Netherlands) to validate four specific risk scores (DIVERT, CARS, EARLI and previous acute admissions) and three frailty indicators (CHESS, Fried Frailty Criteria and Frailty Index). Outcome measures were unplanned hospital admissions, ED visits or any unplanned hospital visits after 6 months. Missing data were handled by multiple imputation. Performance was determined by assessing calibration and discrimination (area under receiver operating characteristic curve (AUC)).
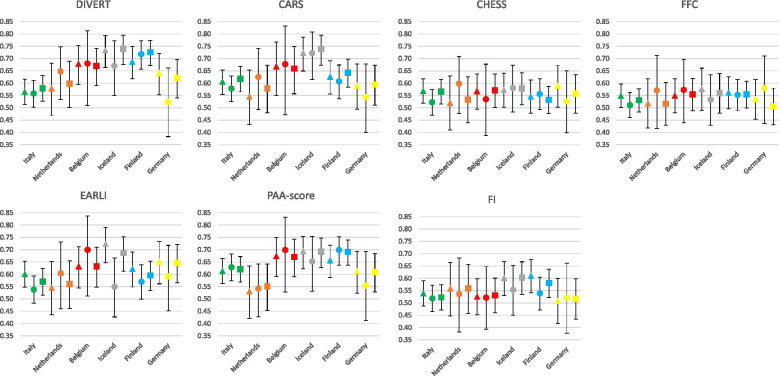
Risk score performance varied across countries. In Iceland, for any unplanned hospital visits DIVERT and CARS reached a fair predictive value (AUC 0.74 [0.68-0.80] and AUC 0.74 [0.67-0.80]), respectively). In Finland, DIVERT had fair performance predicting ED visits (AUC 0.72 [0.67-0.77]) and any unplanned hospital visits (AUC 0.73 [0.67-0.77]). In other countries, AUCs did not exceed 0.70.
Geographical validation of risk scores predicting unplanned hospital visits in home care recipients showed substantial variations of poor to fair performance across countries. Unplanned hospital visits seem considerably dependent on healthcare context. Therefore, risk scores should be validated regionally before applied to practice. Future studies should focus on identification of more discriminative predictors in order to develop more accurate risk scores.
准确识别有计划外住院风险的老年人有助于实施预防干预措施。已经开发出几种风险评分来识别有计划外住院风险的老年人。尚不清楚在一个国家开发的风险评分在另一个国家的表现是否相同。本研究验证了七种风险评分,以预测来自六个国家的老年家庭护理接受者的计划外住院和急诊部(ED)就诊。
我们使用了 IBenC 样本(n=2446),这是来自六个国家(比利时、芬兰、德国、冰岛、意大利和荷兰)的老年家庭护理接受者队列,以验证四种特定的风险评分(DIVERT、CARS、EARLI 和先前的急性入院)和三种脆弱性指标(CHESS、Fried 脆弱性标准和脆弱性指数)。结果测量是 6 个月后计划外住院、ED 就诊或任何计划外住院就诊。通过多次插补处理缺失数据。通过评估校准和区分度(接受者操作特征曲线下的面积(AUC))来确定性能。
风险评分的性能在不同国家之间有所不同。在冰岛,对于任何计划外住院就诊,DIVERT 和 CARS 分别达到了良好的预测值(AUC 为 0.74 [0.68-0.80]和 AUC 为 0.74 [0.67-0.80])。在芬兰,DIVERT 对 ED 就诊(AUC 为 0.72 [0.67-0.77])和任何计划外住院就诊(AUC 为 0.73 [0.67-0.77])具有良好的预测性能。在其他国家,AUC 均未超过 0.70。
在家庭护理接受者中预测计划外住院就诊的风险评分的地理验证表明,不同国家之间的性能差异很大,从较差到良好不等。计划外住院就诊似乎在很大程度上取决于医疗保健环境。因此,在应用于实践之前,风险评分应在区域内进行验证。未来的研究应侧重于识别更具区分度的预测因子,以开发更准确的风险评分。