Men's Health Foundation, Los Angeles, California.
Broward Health Medical Center, Fort Lauderdale, Florida.
AIDS. 2022 Feb 1;36(2):195-203. doi: 10.1097/QAD.0000000000003085.
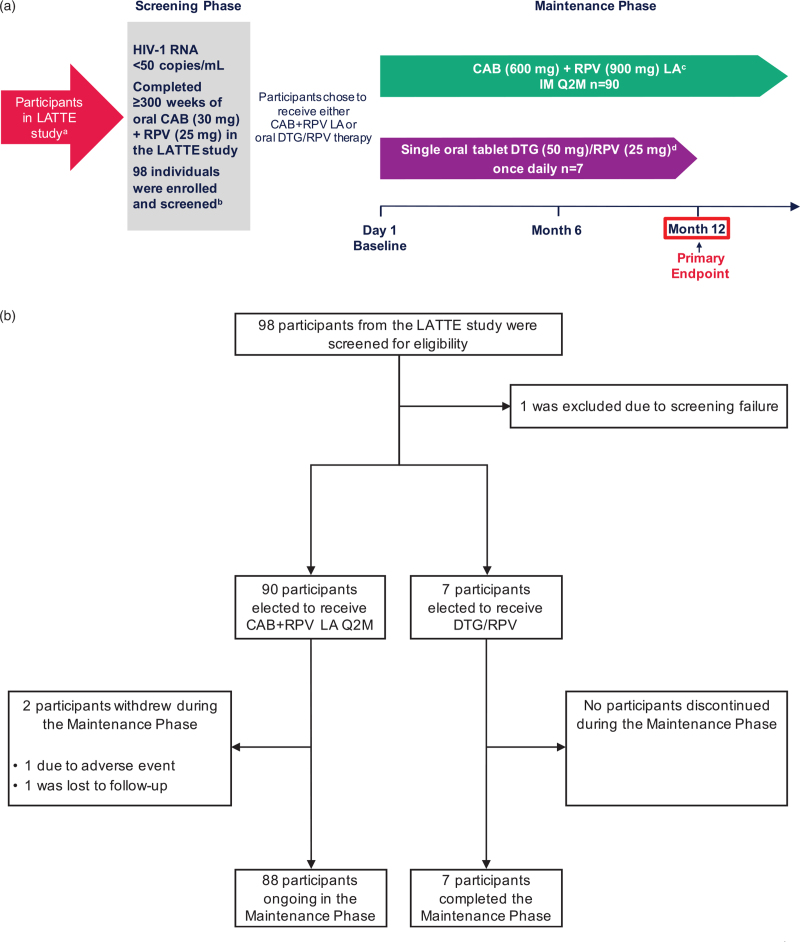
Long-acting formulations of cabotegravir (CAB) and rilpivirine (RPV) have demonstrated efficacy in Phase 3 studies. POLAR (NCT03639311) assessed antiviral activity and safety of CAB+RPV long-acting administered every 2 months (Q2M) in adults living with HIV-1 who previously received daily oral CAB+RPV in LATTE (NCT01641809).
A Phase 2b, multicenter, open-label, rollover study.
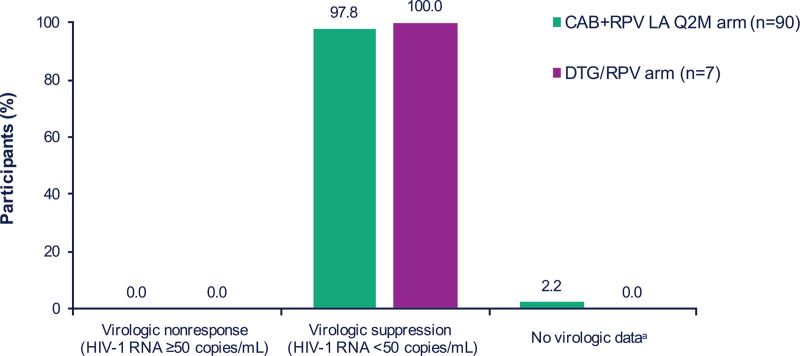
LATTE participants with plasma HIV-1 RNA less than 50 copies/ml who completed at least 300 weeks on study were eligible. Participants elected to switch to either CAB+RPV long-acting Q2M or daily oral dolutegravir/RPV for maintenance of virologic suppression. The primary endpoint was the proportion of participants with HIV-1 RNA greater than or equal to 50 copies/ml at Month 12 (M12) per the Food and Drug Administration Snapshot algorithm. The incidence of confirmed virologic failure (CVF, two consecutive HIV-1 RNA measurements greater than or equal to 200 copies/ml), as well as safety, laboratory, and patient-reported outcomes (HIV Treatment Satisfaction and preference questionnaires) were also assessed.
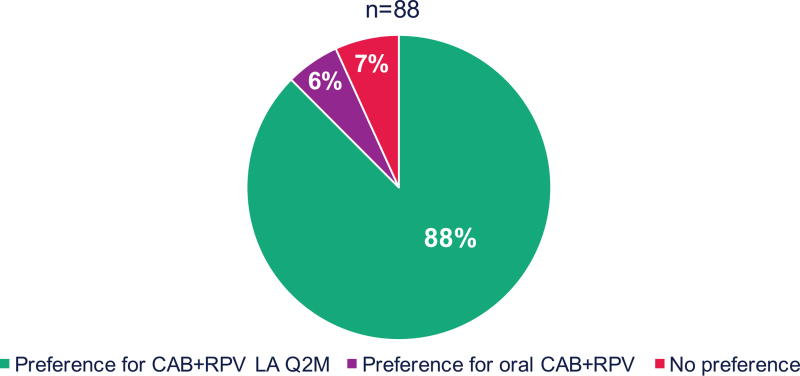
Of 97 participants enrolled, 90 chose to receive CAB+RPV long-acting and seven chose dolutegravir/RPV. At M12, no participant had HIV-1 RNA greater than or equal to 50 copies/ml or met the CVF criterion in either treatment group. No new safety signals were identified. Total treatment satisfaction was high at Baseline and remained stable through M12 across both treatment groups. Overall, 88% (n = 77/88) of long-acting arm participants preferred CAB+RPV long-acting to oral CAB+RPV.
CAB+RPV long-acting maintained virologic suppression in participants who had previously received daily oral CAB+RPV for at least 5 years in LATTE, with a favorable safety profile. Most participants preferred CAB+RPV long-acting to their prior oral CAB+RPV regimen at M12.
长效卡替拉韦(CAB)和利匹韦林(RPV)制剂在 3 期研究中显示出疗效。POLAR(NCT03639311)评估了先前接受每日口服 CAB+RPV 的 HIV-1 成人中,每 2 个月(Q2M)给予 CAB+RPV 长效制剂的抗病毒活性和安全性。
一项 2b 期、多中心、开放性、滚降研究。
LATTE 参与者的血浆 HIV-1 RNA 小于 50 拷贝/ml,完成至少 300 周的研究后符合条件。参与者选择转换为 CAB+RPV 长效 Q2M 或每日口服多拉韦林/RPV 以维持病毒学抑制。主要终点是根据食品和药物管理局快照算法,在第 12 个月(M12)时 HIV-1 RNA 大于或等于 50 拷贝/ml 的参与者比例。还评估了确认的病毒学失败(CVF,两次连续 HIV-1 RNA 测量大于或等于 200 拷贝/ml)的发生率以及安全性、实验室和患者报告的结果(HIV 治疗满意度和偏好问卷)。
97 名入组参与者中,90 名选择接受 CAB+RPV 长效治疗,7 名选择多拉韦林/RPV。在 M12 时,两组治疗中均没有参与者的 HIV-1 RNA 大于或等于 50 拷贝/ml 或符合 CVF 标准。未发现新的安全信号。两组基线时的总治疗满意度均较高,在 M12 时保持稳定。总体而言,长效组 88%(n=77/88)的参与者更喜欢长效 CAB+RPV 优于口服 CAB+RPV。
在 LATTE 中,先前接受每日口服 CAB+RPV 至少 5 年的参与者中,CAB+RPV 长效制剂维持了病毒学抑制,安全性良好。大多数参与者在 M12 时更喜欢长效 CAB+RPV 而不是其先前的口服 CAB+RPV 方案。