Department of Emergency and Critical Care Medicine, Hitachi General Hospital, Hitachi, Ibaraki, Japan.
Critical Care Research Group, Faculty of Medicine, University of Queensland and the Prince Charles Hospital, Brisbane, Australia.
Clin Nutr. 2022 Dec;41(12):2947-2954. doi: 10.1016/j.clnu.2021.09.033. Epub 2021 Sep 27.
BACKGROUND & AIMS: Nutrition therapy for Intensive Care Unit (ICU) patients involves complex decision-making, especially during the COVID-19 pandemic. We investigated the use of nutrition therapy in ICU patients with and without COVID-19 infections.
Nutrition therapy was evaluated during a world-wide one-day prevalence study focused on implementation of the ABCDEF bundle (A: regular pain assessment, B: both spontaneous awakening and breathing trials, C: regular sedation assessment, D: regular delirium assessment, E: early mobility and exercise, and F: family engagement and empowerment) during the COVID-19 pandemic. Basic ICU and patient demographics including nutrition therapy delivery were collected on the survey day. Physical activity for patients with and without COVID infections was categorized using the ICU mobility scale (IMS). Multivariable regression analysis of nutrition was conducted using ICU parameters.
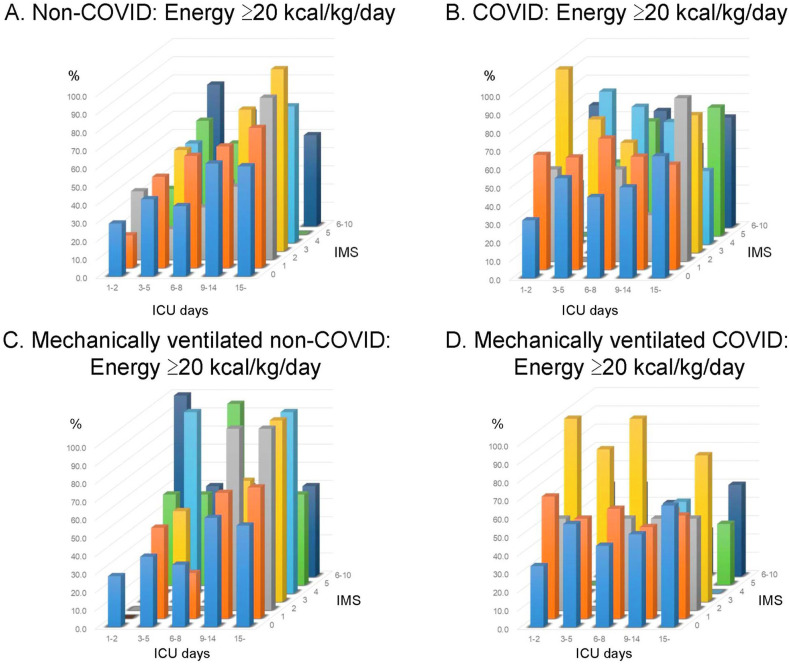
The survey included 627 non-COVID and 602 COVID patients. A higher proportion of COVID-19 patients received energy ≥20 kcal/kg/day (55% vs. 45%; p = 0.0007) and protein ≥1.2 g/kg/day (45% vs. 35%; p = 0.0011) compared to non-COVID patients. Enteral nutrition was provided to most COVID patients even with prone positioning (91%). Despite nutrition therapy, IMS was extremely low in both groups; median IMS was 1 in non-COVID patients and 0 in COVID patients. The rate of energy delivery ≥20 kcal/kg/day was significantly higher in patients with COVID-19 infections in the subgroup of ICU days ≤5 days and IMS ≤2. Having a dedicated ICU nutritionist/dietitian was significantly associated with appropriate energy delivery in patients both with and without COVID-19 infections, but not with protein delivery.
During the COVID-19 pandemic, patients with COVID-19 infections received higher energy and protein delivery. Generally low mobility levels highlight the need to optimize early mobilization with nutrition therapy in all ICU patients.
重症监护病房(ICU)患者的营养治疗涉及复杂的决策,尤其是在 COVID-19 大流行期间。我们调查了 COVID-19 感染和非 COVID-19 感染的 ICU 患者的营养治疗使用情况。
在一项全球性的 ICU 患者营养治疗评估研究中,在 COVID-19 大流行期间,重点评估 ABCDEF 捆绑包(A:定期疼痛评估,B:自主觉醒和呼吸试验,C:定期镇静评估,D:定期谵妄评估,E:早期活动和运动,F:家庭参与和授权)的实施情况。在调查当天收集了基本的 ICU 和患者人口统计学数据,包括营养治疗的实施情况。对有和没有 COVID 感染的患者的身体活动情况,使用 ICU 活动量表(IMS)进行分类。使用 ICU 参数对营养进行多变量回归分析。
该调查包括 627 例非 COVID 患者和 602 例 COVID 患者。与非 COVID 患者相比,COVID-19 患者接受能量≥20 kcal/kg/天(55%比 45%;p=0.0007)和蛋白质≥1.2 g/kg/天(45%比 35%;p=0.0011)的比例更高。即使在俯卧位时,大多数 COVID 患者也接受了肠内营养(91%)。尽管进行了营养治疗,但两组的 IMS 都极低;非 COVID 患者的 IMS 中位数为 1,COVID 患者的 IMS 中位数为 0。在 ICU 入住天数≤5 天和 IMS≤2 的亚组中,COVID-19 感染患者的能量供给率≥20 kcal/kg/天显著更高。有专门的 ICU 营养师/营养师与 COVID-19 感染和非 COVID-19 感染患者的能量供给显著相关,但与蛋白质供给无关。
在 COVID-19 大流行期间,COVID-19 感染患者接受了更高的能量和蛋白质供给。一般来说,活动水平较低突出表明需要在所有 ICU 患者中通过营养治疗优化早期活动。