Division of Vascular Surgery and Endovascular Therapy, Department of Surgery, Hospital of the University of Pennsylvania, Philadelphia, PA.
Renal, Electrolyte and Hypertension Division, University of Pennsylvania, Philadelphia, PA; Center for Clinical Epidemiology and Biostatistics, University of Pennsylvania, Philadelphia, PA.
Ann Vasc Surg. 2022 Mar;80:196-205. doi: 10.1016/j.avsg.2021.07.057. Epub 2021 Oct 14.
The association between socioeconomic factors and development of peripheral artery disease (PAD) has not been as well characterized compared to other cardiovascular diseases. We sought to define how annual income, sex, race, and education level are associated with newly diagnosed PAD in a well-characterized, diverse set of adults with CKD.
The Chronic Renal Insufficiency Cohort Study (CRIC) is a multicenter, prospective cohort study designed to examine risk factors for progression of CKD and cardiovascular disease. Demographic and clinical data including ankle brachial index (ABI) and interventions were collected at baseline, as well as yearly during follow-up visits. Annual income was categorized as: <$25,000, $25,000-50,000, $50,000-100,000, or above $100,000. We excluded those with pre-existing PAD, defined as enrollment ABI of <0.9 or >1.4, or missing income data. Cox proportional hazards regression was used to estimate the risk for incident PAD during CRIC enrollment, defined as a drop in ABI to <0.90 or a confirmed PAD intervention, including revascularization or amputation.
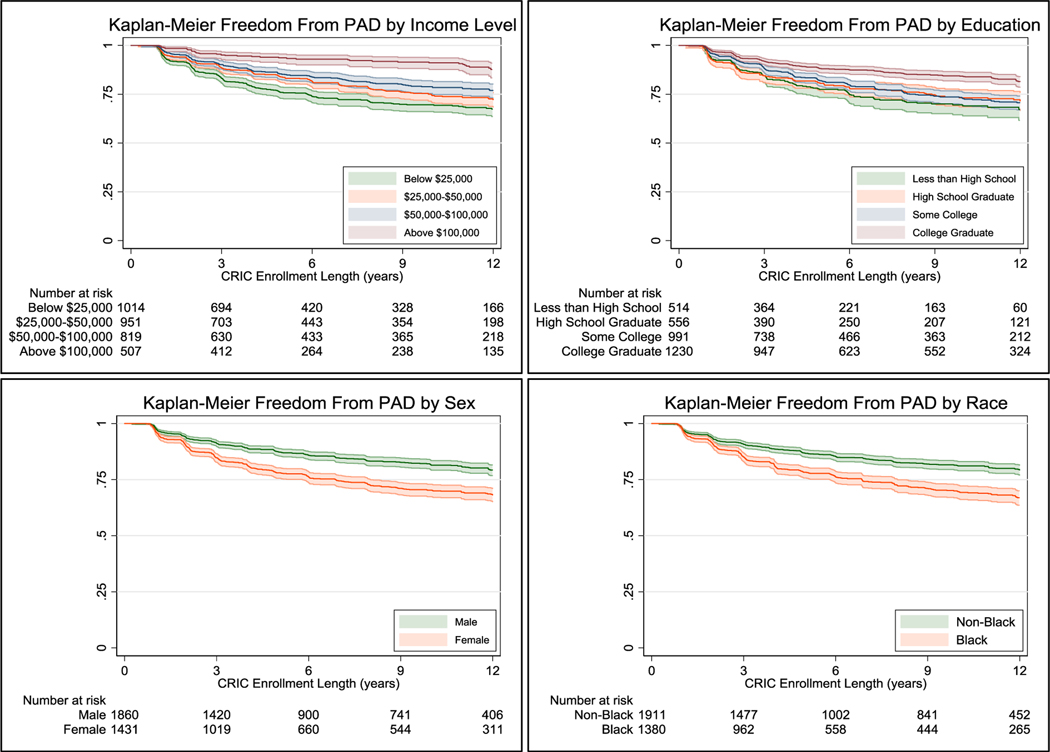
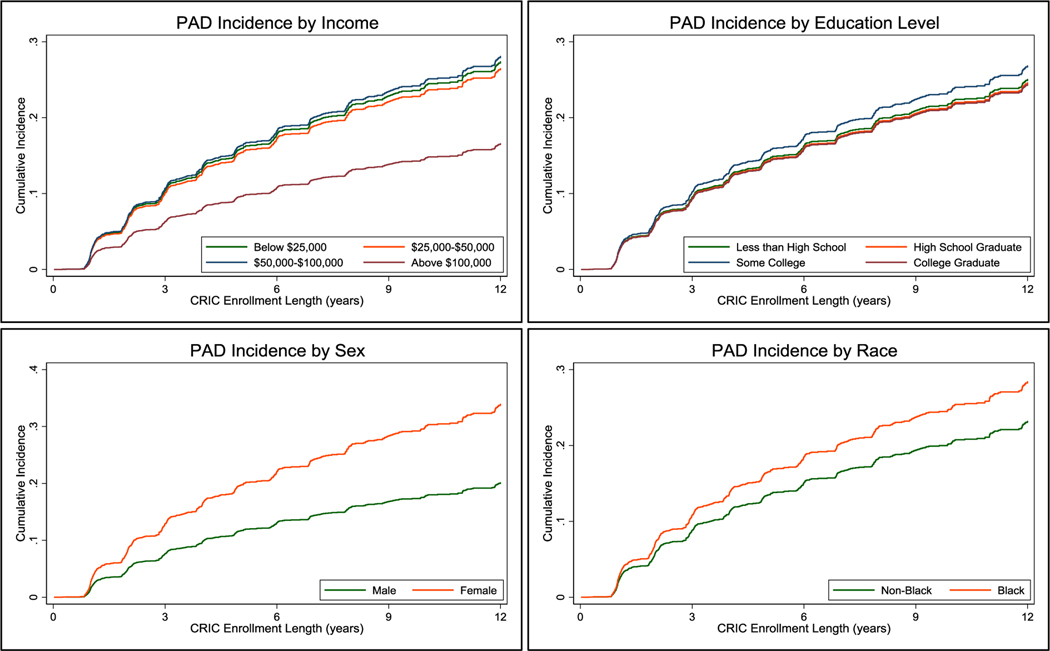
A total of 3,313 patients met inclusion criteria, the mean age was 58.7 years, 56% were male, and 42% were Black. Over a median follow-up of 10.1 years, 639 participants (19%) were newly diagnosed with PAD. After adjusting for cardiovascular risk factors, all lower levels of annual household income were associated with increased incidence of PAD (income <$25,000 HR 1.7, 95% CI 1.1-2.4, P = 0.008; income $25,000-50,000 HR 1.5, 95% CI 1.1-2.3, P = 0.009; income $50,000-100,000 HR 1.6, 95% CI 1.2-2.4, P = 0.004), relative to a baseline annual income of >$100,000 (overall P-value = 0.02). In the multivariable model, there was no association between education level and PAD incidence (P = 0.80). Black race (HR 1.2, 95% CI 1.0-1.5, P = 0.023) and female sex (HR 1.7, 95% CI 1.4-2.0, P < 0.001) were independently associated with PAD incidence. Multiple imputation analysis provided similar results.
In the CRIC, a multi-center cohort of prospectively followed CKD patients undergoing yearly CVD surveillance, lower annual household income, female sex, and Black race were significantly associated with the PAD incidence. In contrast, level of education was not independently associated with incident PAD.
与其他心血管疾病相比,社会经济因素与外周动脉疾病(PAD)发展之间的关系尚未得到很好的描述。我们旨在明确年收入、性别、种族和教育水平如何与在一组特征明确、多样化的慢性肾脏病(CKD)患者中新诊断的 PAD 相关。
慢性肾脏不全队列研究(CRIC)是一项多中心、前瞻性队列研究,旨在研究 CKD 和心血管疾病进展的危险因素。在基线以及随访期间的每年就诊时,收集人口统计学和临床数据,包括踝臂指数(ABI)和干预措施。年收入分为:<$25,000、$25,000-50,000、$50,000-100,000 或>$100,000。我们排除了那些有预先存在的 PAD 的患者,定义为入组时 ABI <0.9 或>1.4,或缺失收入数据。使用 Cox 比例风险回归估计 CRIC 入组时新发 PAD 的风险,新发 PAD 定义为 ABI 下降至<0.90 或确认 PAD 干预,包括血运重建或截肢。
共有 3313 名患者符合纳入标准,平均年龄为 58.7 岁,56%为男性,42%为黑人。在中位随访 10.1 年期间,639 名参与者(19%)新诊断为 PAD。在校正心血管危险因素后,所有较低水平的年收入与 PAD 发生率的增加相关(年收入<$25,000 HR 1.7,95%CI 1.1-2.4,P=0.008;年收入 $25,000-50,000 HR 1.5,95%CI 1.1-2.3,P=0.009;年收入 $50,000-100,000 HR 1.6,95%CI 1.2-2.4,P=0.004),与基线年收入>$100,000 相比(整体 P 值=0.02)。在多变量模型中,教育水平与 PAD 发生率之间没有关联(P=0.80)。黑种人(HR 1.2,95%CI 1.0-1.5,P=0.023)和女性(HR 1.7,95%CI 1.4-2.0,P<0.001)与 PAD 发生率独立相关。多重插补分析提供了类似的结果。
在 CRIC 中,对一组接受每年 CVD 监测的特征明确的 CKD 患者进行的多中心队列研究中,较低的家庭年收入、女性和黑种人种族与 PAD 发生率显著相关。相比之下,教育水平与新发 PAD 无独立相关性。