Liu Chengzhe, Yu Zhiyao, Chen Huaqiang, Wang Jun, Liu Wei, Zhou Liping, Wang Yueyi, Chen Hu, Zhou Huixin, Liu Zhihao, Han Jiapeng, Jiang Hong, Yu Lilei
Department of Cardiology, Renmin Hospital of Wuhan University, Wuhan, China.
Cardiac Autonomic Nervous System Research Center of Wuhan University, Wuhan, China.
Front Cardiovasc Med. 2021 Sep 29;8:714276. doi: 10.3389/fcvm.2021.714276. eCollection 2021.
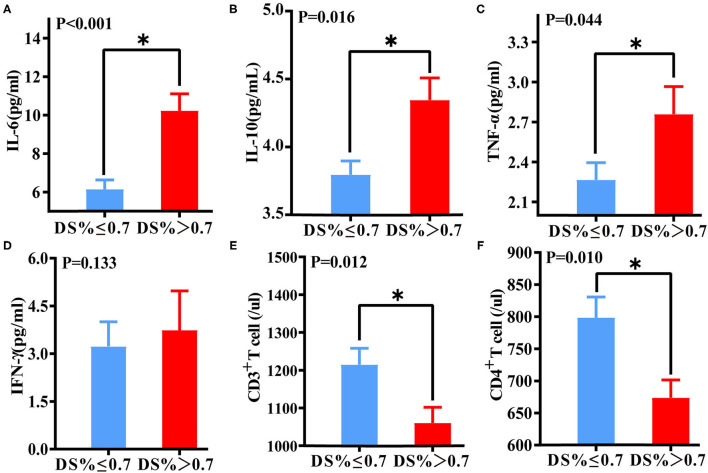
The association between coronary physiology and immunoinflammation has not been investigated. We performed a retrospective study using quantitative flow ratio (QFR) to evaluate the interaction between immunoinflammatory biomarkers and coronary physiology. A total of 172 patients with CAD who underwent coronary arteriography (CAG) and QFR were continuously enrolled from May 2020 to February 2021. As a quantitative indicator of coronary physiology, QFR can reflect the functional severity of coronary artery stenosis. The target vessel measured by QFR was defined as that with the most severe lesions. Significant coronary anatomical stenosis was defined as 70% stenosis in the target vessel. Compared with the QFR > 0.8 group, interleukin (IL)-6, IL-10, tumor necrosis factor (TNF)-α, and interferon (IFN)-γ were increased and CD3 and CD4 T lymphocyte counts were decreased in the QFR ≤ 0.8 group. In addition, patients with DS ≤ 70% had higher IL-6, IL-10, and TNF-α levels and decreased CD3 and CD4 T lymphocyte counts than those with DS > 70%. Logistic regression analysis indicated IL-6 to be an independent predictor of significant coronary functional and anatomic stenosis (odds ratio, 1.125; 95% CI, 1.059-1.196; < 0.001). Receiver operating characteristic (ROC) analyses showed that IL-6 > 6.36 was predictive of QFR ≤ 0.8 of the target vessel. The combination of IL-6, IL-10 and CD4 improved the value for predicting QFR ≤ 0.8 of the target vessel (AUC, 0.737; 95% CI, 0.661-0.810). Among immunoinflammatory biomarkers, IL-6 was independently associated with a higher risk of QFR ≤ 0.8 of the target vessel. The combination of immunoinflammatory biomarkers was highly predictive of significant coronary functional and anatomic stenosis.
冠状动脉生理学与免疫炎症之间的关联尚未得到研究。我们进行了一项回顾性研究,使用定量血流比(QFR)来评估免疫炎症生物标志物与冠状动脉生理学之间的相互作用。从2020年5月至2021年2月,连续纳入了172例行冠状动脉造影(CAG)和QFR检查的冠心病患者。作为冠状动脉生理学的定量指标,QFR可以反映冠状动脉狭窄的功能严重程度。QFR测量的目标血管定义为病变最严重的血管。显著冠状动脉解剖狭窄定义为目标血管狭窄70%。与QFR>0.8组相比,QFR≤0.8组的白细胞介素(IL)-6、IL-10、肿瘤坏死因子(TNF)-α和干扰素(IFN)-γ升高,CD3和CD4 T淋巴细胞计数降低。此外,与病变严重程度(DS)>70%的患者相比,DS≤70%的患者IL-6、IL-10和TNF-α水平更高,CD3和CD4 T淋巴细胞计数降低。逻辑回归分析表明,IL-6是冠状动脉显著功能和解剖狭窄的独立预测因子(优势比,1.125;95%可信区间,1.059-1.196;P<0.001)。受试者工作特征(ROC)分析表明,IL-6>6.36可预测目标血管QFR≤0.8。IL-6、IL-10和CD4的联合使用提高了预测目标血管QFR≤0.8的价值(曲线下面积,0.737;95%可信区间,0.661-0.810)。在免疫炎症生物标志物中,IL-6与目标血管QFR≤0.8的较高风险独立相关。免疫炎症生物标志物的联合使用对显著冠状动脉功能和解剖狭窄具有高度预测性。