Wang Jun, Liu Chengzhe, Guo Fuding, Zhou Zhen, Zhou Liping, Wang Yueyi, Chen Huaqiang, Zhou Huixin, Liu Zhihao, Duan Shoupeng, Sun Ji, Deng Qiang, Xu Saiting, Jiang Hong, Yu Lilei
Department of Cardiology, Renmin Hospital of Wuhan University, Wuhan, China.
Cardiac Autonomic Nervous System Research Centre of Wuhan University, Wuhan, China.
Front Cardiovasc Med. 2022 Mar 22;9:848499. doi: 10.3389/fcvm.2022.848499. eCollection 2022.
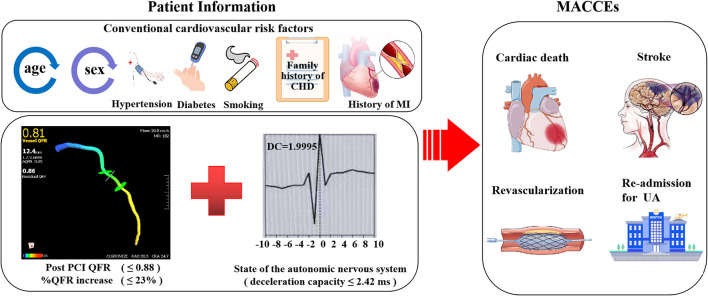
Both coronary physiology and deceleration capacity (DC) showed prognostic efficacy for patients with acute coronary syndrome (ACS). This retrospective cohort study was performed to evaluate the prognostic implication of DC combined with the relative increase and final coronary physiology as detected by quantitative flow ratio (QFR) for patients with non-ST-elevation ACS (NSTE-ACS) who underwent complete and successful percutaneous coronary intervention (PCI).
Patients with NSTE-ACS who underwent PCI with pre- and post-procedural QFR in our department between January 2018 and November 2019 were included. The 24-hour deceleration capacity (DC 24h) was obtained Holter monitoring. The incidence of major adverse cardiac and cerebrovascular events (MACCEs) during follow up was defined as the primary outcome. The optimal cutoffs of the relative increase, final QFR, and DC 24h for prediction of MACCEs were determined receiver operating characteristic (ROC) analysis and the predictive efficacies were evaluated with multivariate Cox regression analysis.
Overall, 240 patients were included. During a mean follow up of 21.3 months, 31 patients had MACCEs. Results of multivariate Cox regression analyses showed that a higher post-PCI QFR [adjusted hazard ratio (HR): 0.318; 95% confidence interval (CI): 0.129-0.780], a higher relative QFR increase (HR: 0.161; 95% CI: 0.066-0.391], and a higher DC (HR: 0.306; 95% CI: 0.134-0.701) were all independent predictors of lower risk of MACCEs. Subsequently, incorporating low DC (≤2.42) into the risk predicting model with clinical variables, the predictive efficacies of low relative QRS increase (≤23%) and low post-PCI QFR (≤0.88) for MACCEs were both significantly improved.
The DC combined with relative increase and final coronary physiology may improve the predictive efficacy of existing models based on clinical variables for MACCEs in NSTE-ACS patients who underwent complete and successful PCI.
冠状动脉生理学和减速能力(DC)对急性冠状动脉综合征(ACS)患者均显示出预后评估价值。本回顾性队列研究旨在评估DC联合定量血流比率(QFR)检测的相对增加量和最终冠状动脉生理学指标,对接受了完整且成功的经皮冠状动脉介入治疗(PCI)的非ST段抬高型ACS(NSTE-ACS)患者的预后意义。
纳入2018年1月至2019年11月期间在我科接受PCI且术前和术后均有QFR检测的NSTE-ACS患者。通过动态心电图监测获得24小时减速能力(DC 24h)。将随访期间主要不良心脑血管事件(MACCE)的发生率定义为主要结局。通过受试者工作特征(ROC)分析确定相对增加量、最终QFR和DC 24h预测MACCE的最佳截断值,并采用多变量Cox回归分析评估预测效能。
共纳入240例患者。在平均21.3个月的随访期间,31例患者发生了MACCE。多变量Cox回归分析结果显示,PCI术后较高的QFR[调整后风险比(HR):0.318;95%置信区间(CI):0.129 - 0.780]、较高的QFR相对增加量(HR:0.161;95% CI:0.066 - 0.39)和较高的DC(HR:0.306;95% CI:0.134 - 0.701)均是MACCE低风险的独立预测因素。随后,将低DC(≤2.42)纳入包含临床变量的风险预测模型中,低QRS相对增加量(≤23%)和低PCI术后QFR(≤0.88)对MACCE的预测效能均显著提高。
DC联合相对增加量和最终冠状动脉生理学指标,可能会提高基于临床变量的现有模型对接受了完整且成功PCI的NSTE-ACS患者MACCE的预测效能。