Sinclair SaTia T, Orr Melissa N, Rothfusz Christopher A, Klika Alison K, McLaughlin John P, Piuzzi Nicolas S
Department of Orthopaedic Surgery, Cleveland Clinic Foundation, Cleveland, OH, USA.
Arthroplast Today. 2021 Oct 4;11:205-211. doi: 10.1016/j.artd.2021.08.019. eCollection 2021 Oct.
In revision total knee arthroplasty (TKA), information regarding perioperative mortality risk is essential for careful decision-making. This study aimed to elucidate the (1) overall 30-day mortality rate and (2) 30-day mortality rate stratified by age, comorbidity, and septic vs aseptic failure after revision TKA.
The American College of Surgeons National Surgical Quality Improvement Program was reviewed for all patients undergoing revision TKA from 2011 to 2019. A total of 32,354 patients who underwent TKA were identified and categorized as mortality (n = 115) or mortality-free (n = 32,239). Patient characteristics were compared between cohorts and further stratified by septic and aseptic failure.
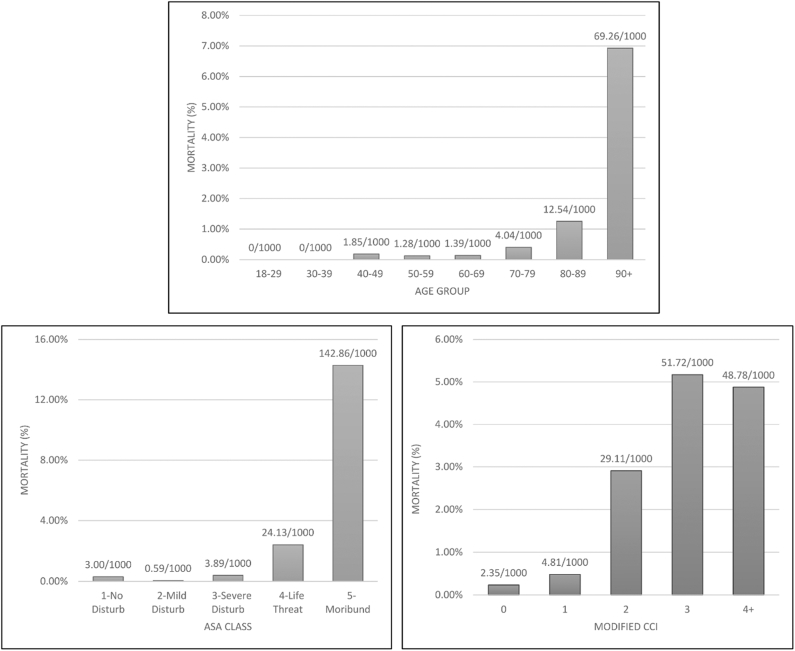
The overall 30-day mortality rate was 0.36%. The percentage of deaths per age group (normalized per 1000) was 0% (18-29 years), 0% (30-39 years), 0.18% (40-49 years), 0.13% (50-59 years), 0.14% (60-69 years), 0.40% (70-79 years), 1.25% (80-89 years), and 6.93% (90+ years). The percentage of deaths per American Society of Anesthesiologists (ASA) class was 0.30% (ASA 1), 0.06% (ASA 2), 0.39% (ASA 3), 2.41% (ASA 4), and 14.29% (ASA 5). Septic revision ( < .001), general anesthesia ( < .001), body mass index ≤ 24.9 ( < .001), and insulin-dependent diabetes ( = .039) were associated with an increased risk of mortality.
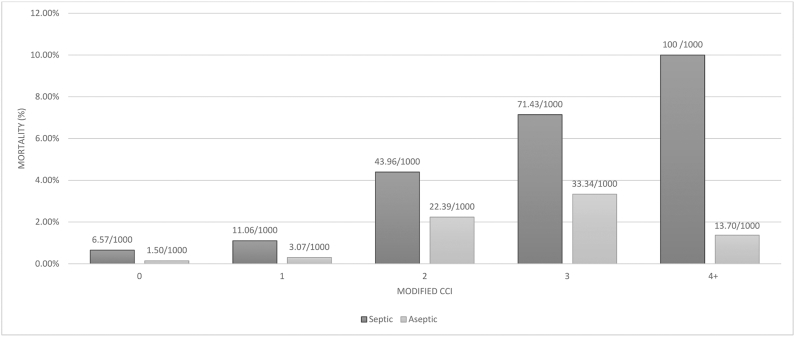
Increasing age, greater comorbidity burden, underweight or normal body mass index, insulin-dependent diabetes, septic revision, and general anesthesia were all associated with an increased risk of mortality after revision TKA. Notably, 1 in 80 patients aged 80-89 years died after revision TKA compared to 1 in 720 patients aged 60-69 years. Patients who underwent septic revision had a 4-fold increase in mortality compared to aseptic revision. Our stratified assessment of mortality provides a more individualized estimation of risk that can be used for patient counseling in revision TKA.
在全膝关节置换翻修术(TKA)中,围手术期死亡风险信息对于谨慎决策至关重要。本研究旨在阐明(1)总体30天死亡率,以及(2)全膝关节置换翻修术后按年龄、合并症、感染性与无菌性失败分层的30天死亡率。
回顾美国外科医师学会国家外科质量改进计划中2011年至2019年接受全膝关节置换翻修术的所有患者。共识别出32354例行全膝关节置换术的患者,并分为死亡组(n = 115)和非死亡组(n = 32239)。比较两组患者的特征,并按感染性和无菌性失败进一步分层。
总体30天死亡率为0.36%。各年龄组的死亡百分比(每1000人标准化)分别为0%(18 - 29岁)、0%(30 - 39岁)、0.18%(40 - 49岁)、0.13%(50 - 59岁)、0.14%(60 - 69岁)、0.40%(70 - 79岁)、1.25%(80 - 89岁)和6.93%(90岁及以上)。美国麻醉医师协会(ASA)分级的死亡百分比分别为0.30%(ASA 1级)、0.06%(ASA 2级)、0.39%(ASA 3级)、2.41%(ASA 4级)和14.29%(ASA 5级)。感染性翻修(< 0.001)、全身麻醉(< 0.001)、体重指数≤24.9(< 0.001)和胰岛素依赖型糖尿病(P = 0.039)与死亡风险增加相关。
年龄增加、合并症负担加重、体重过轻或正常体重指数、胰岛素依赖型糖尿病、感染性翻修和全身麻醉均与全膝关节置换翻修术后死亡风险增加相关。值得注意的是,80 - 89岁的患者中,每80例全膝关节置换翻修术后有1例死亡,而60 - 69岁的患者中,每720例中有1例死亡。与无菌性翻修相比,接受感染性翻修的患者死亡率增加了4倍。我们对死亡率的分层评估提供了更个体化的风险估计,可用于全膝关节置换翻修术患者的咨询。