Department of Biomedical Engineering, School of Engineering & Applied Science, Yale University, New Haven, Connecticut, USA.
Department of Biomedical Engineering, CARIM School for Cardiovascular Diseases, Maastricht University, Maastricht, The Netherlands.
Am J Hypertens. 2022 Mar 8;35(3):272-280. doi: 10.1093/ajh/hpab168.
Pulse wave velocity (PWV) is blood pressure (BP) dependent, leading to the development of the BP-corrected metrics cardio-ankle vascular index (CAVI) and CAVI0. We aimed to assess risk prediction by heart-to-ankle PWV (haPWV), CAVI, and CAVI0 in a US population.
We included 154 subjects (94.8% male; 47.7% African American) with and without heart failure (HF). Left and right haPWV, CAVI, and CAVI0 were measured with the VaSera 1500N device. We prospectively followed participants for a mean of 2.56 years for the composite endpoint death or HF-related hospital admission (DHFA).
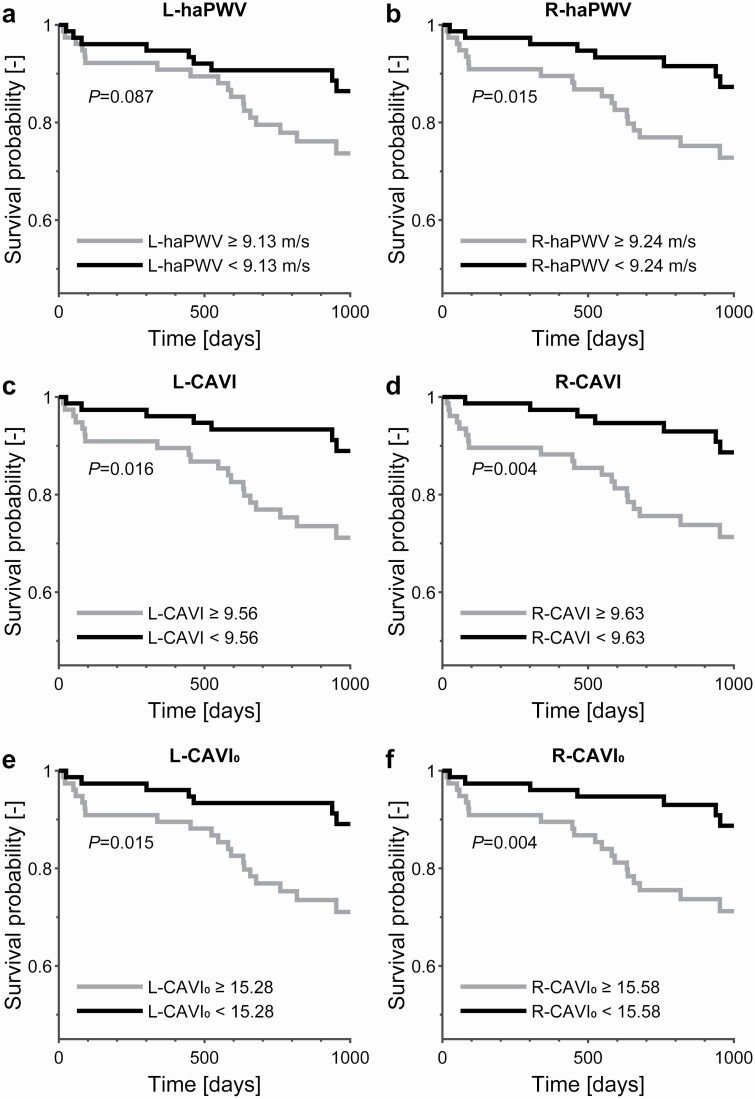
Left and right haPWV, CAVI, and CAVI0 values did not differ significantly. In unadjusted analyses, haPWV (left standardized hazard ratio [HR] = 1.51, P = 0.007; right HR = 1.66, P = 0.003), CAVI (left HR = 1.45, P = 0.012; right HR = 1.58, P = 0.006), and CAVI0 (left HR = 1.39, P = 0.022; right HR = 1.44, P = 0.014) significantly predicted DHFA. Predictive ability showed a decreasing trend from haPWV to CAVI to CAVI0; in line with the increasing amount of BP correction in these metrics. In Cox models, right-sided metrics showed a trend toward stronger predictive ability than left-sided metrics. After adjustment for baseline HF status, the Meta-Analysis Global Group in Chronic Heart Failure (MAGGIC) risk score, and systolic BP, right haPWV (HR = 1.58, P = 0.025) and CAVI (HR = 1.44, P = 0.044), but no other stiffness metrics, remained predictive.
Although conceptually attractive, BP-corrected arterial stiffness metrics do not offer better prediction of DHFA than conventional arterial stiffness metrics, nor do they predict DHFA independently of systolic BP. Our findings support PWV as the primary arterial stiffness metric for outcome prediction.
脉搏波速度(PWV)是血压(BP)依赖性的,这导致了血压校正指标心血管踝臂指数(CAVI)和 CAVI0 的发展。我们旨在评估美国人群中心-踝 PWV(haPWV)、CAVI 和 CAVI0 的风险预测能力。
我们纳入了 154 名受试者(94.8%为男性;47.7%为非裔美国人),其中包括心力衰竭(HF)患者和非 HF 患者。使用 VaSera 1500N 设备测量左、右 haPWV、CAVI 和 CAVI0。我们前瞻性地随访了参与者平均 2.56 年,终点事件为死亡或与 HF 相关的住院(DHFA)。
左、右 haPWV、CAVI 和 CAVI0 值无显著差异。在未经调整的分析中,haPWV(左标准化风险比[HR] = 1.51,P = 0.007;右 HR = 1.66,P = 0.003)、CAVI(左 HR = 1.45,P = 0.012;右 HR = 1.58,P = 0.006)和 CAVI0(左 HR = 1.39,P = 0.022;右 HR = 1.44,P = 0.014)显著预测了 DHFA。预测能力呈现出从 haPWV 到 CAVI 再到 CAVI0 的下降趋势;这与这些指标中血压校正量的增加一致。在 Cox 模型中,右侧指标的预测能力趋势强于左侧指标。在校正基线 HF 状态、MAGGIC 风险评分和收缩压后,右 haPWV(HR = 1.58,P = 0.025)和 CAVI(HR = 1.44,P = 0.044)仍然具有预测能力,但其他僵硬指标没有预测能力。
尽管在概念上具有吸引力,但 BP 校正后的动脉僵硬指标在预测 DHFA 方面并不优于传统的动脉僵硬指标,也不能独立于收缩压预测 DHFA。我们的研究结果支持 PWV 作为主要的动脉僵硬指标用于预测结果。