Clinical Research Division and.
Public Health Services Division, Fred Hutchinson Cancer Research Center, Seattle, WA.
Blood Adv. 2022 Apr 12;6(7):2055-2068. doi: 10.1182/bloodadvances.2020004142.
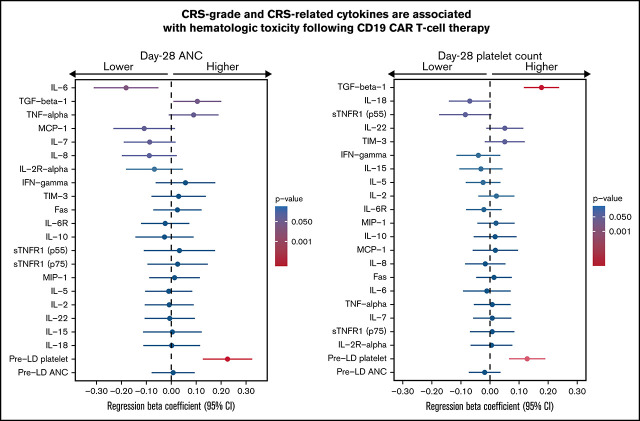
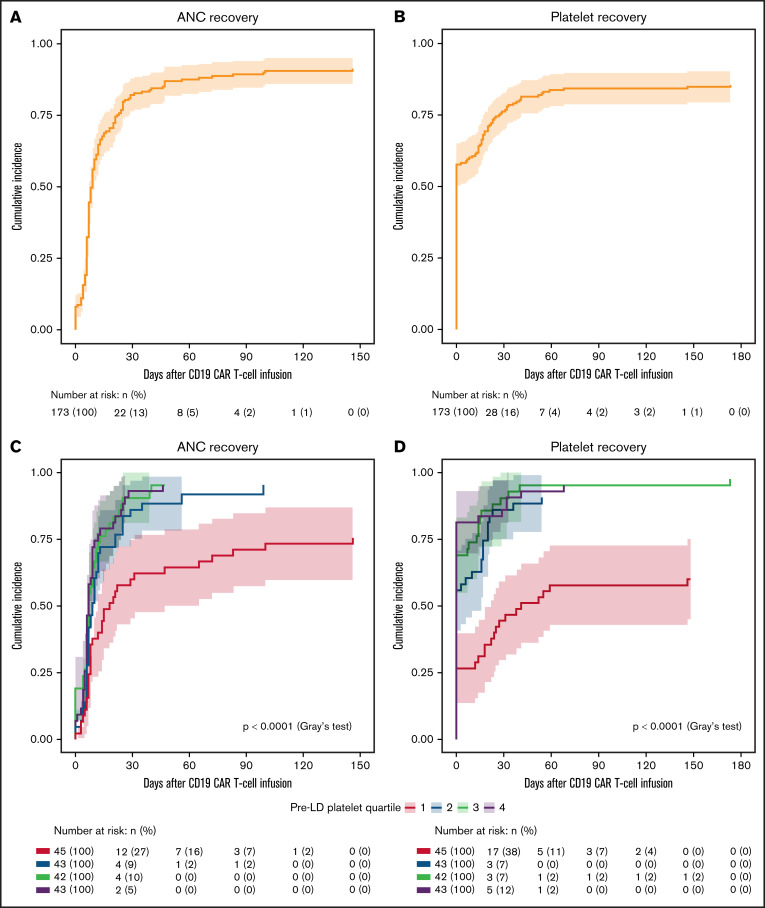
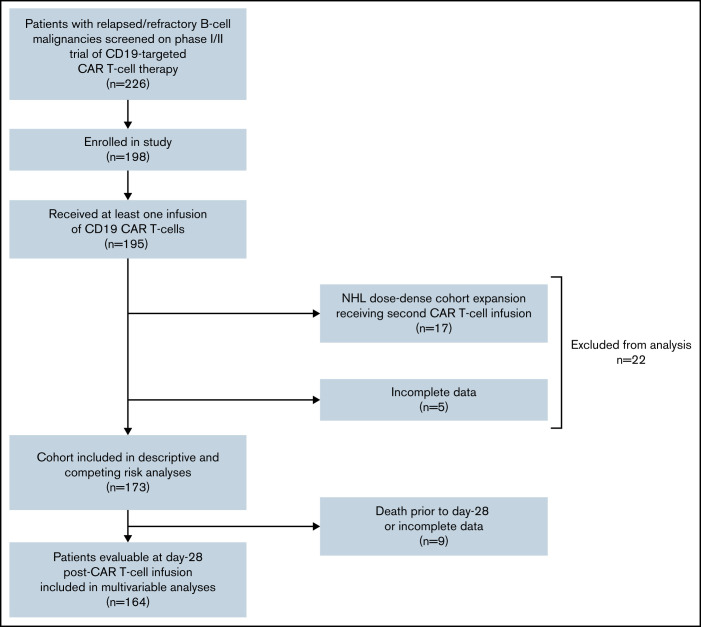
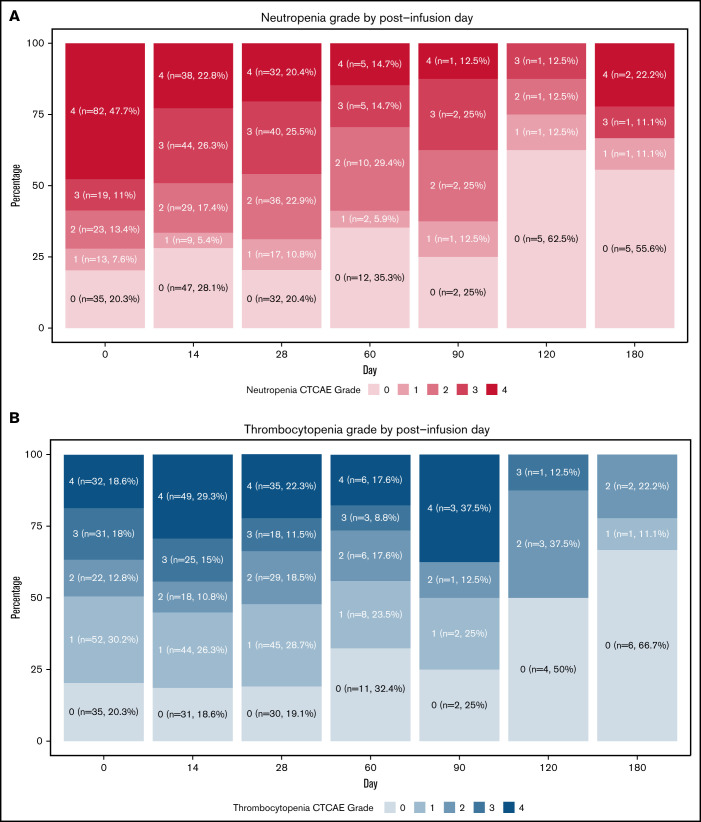
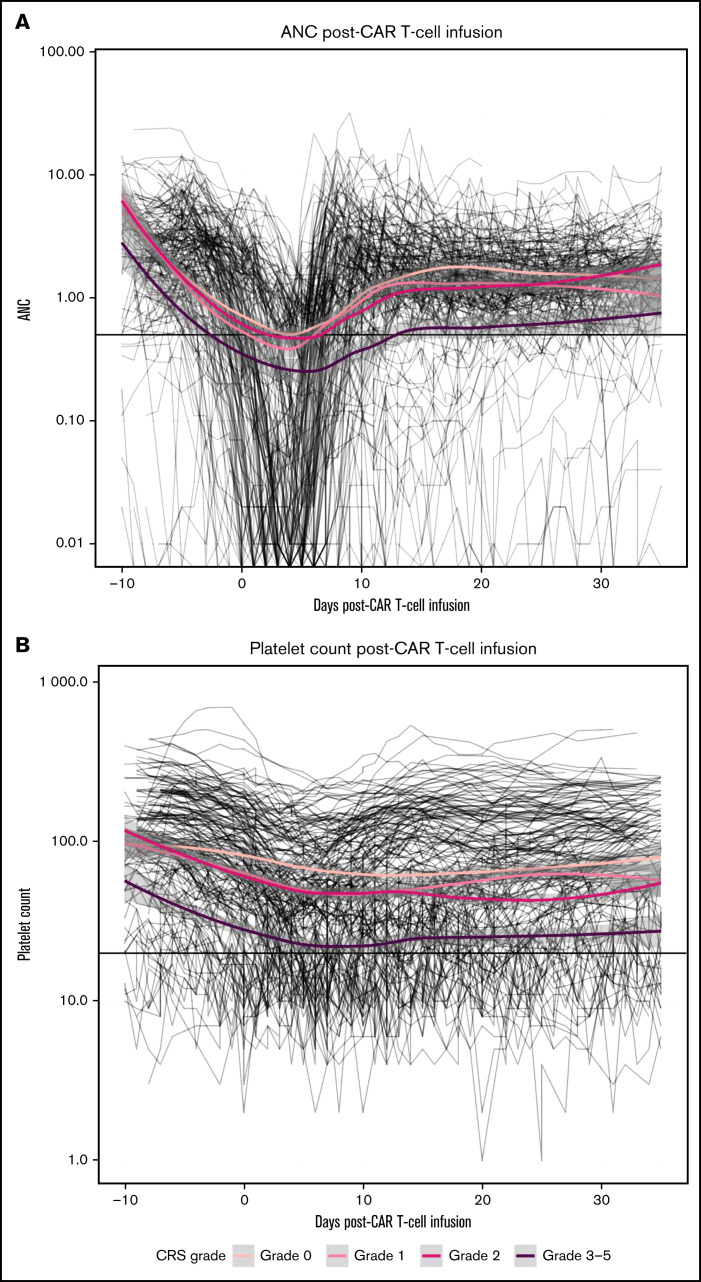
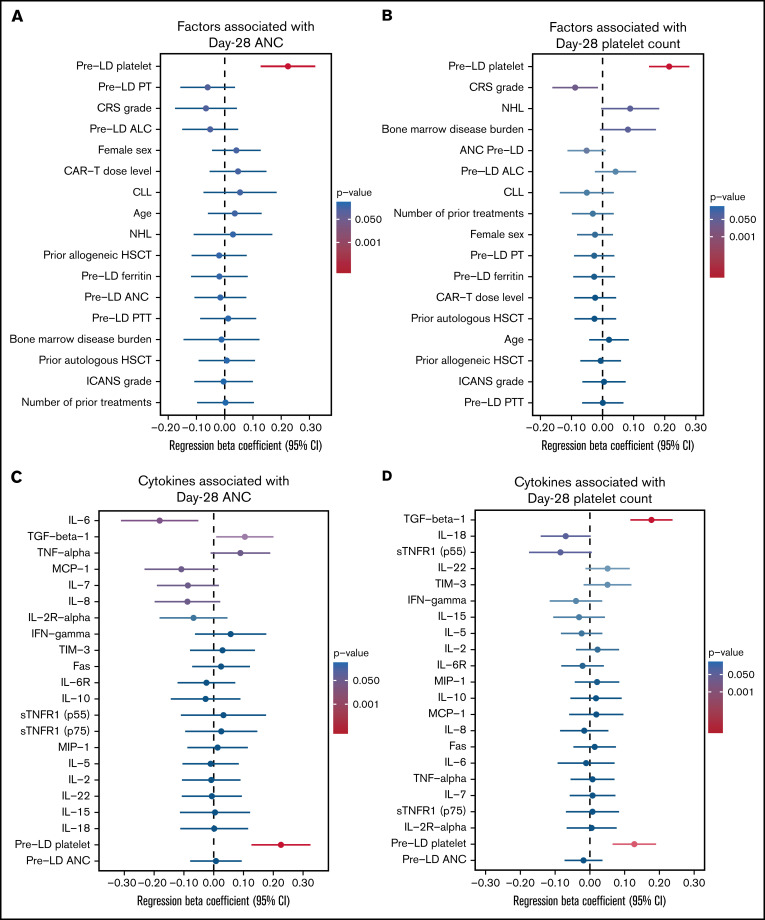
CD19-targeted chimeric antigen receptor (CAR) T-cell therapy has demonstrated remarkable efficacy in patients with relapsed/refractory B-cell malignancies; however, it is associated with toxicities including cytokine release syndrome (CRS), neurotoxicity, and impaired hematopoietic recovery. The latter is associated with high-grade cytopenias requiring extended growth factor or transfusional support, potentially leading to additional complications such as infection or hemorrhage. To date, the factors independently associated with hematologic toxicity have not been well characterized. To address this deficit, we retrospectively analyzed 173 patients who received defined-composition CD19 CAR T-cell therapy in a phase 1/2 clinical trial (https://clinicaltrials.gov; NCT01865617), with primary end points of absolute neutrophil count and platelet count at day-28 after CAR T-cell infusion. We observed cumulative incidences of neutrophil and platelet recovery of 81% and 75%, respectively, at 28 days after infusion. Hematologic toxicity was noted in a significant subset of patients, with persistent neutropenia in 9% and thrombocytopenia in 14% at last follow-up. Using debiased least absolute shrinkage selector and operator regression analysis for high-dimensional modeling and considering patient-, disease-, and treatment-related variables, we identified increased CRS severity as an independent predictor for decreased platelet count and lower prelymphodepletion platelet count as an independent predictor of both decreased neutrophil and platelet counts after CD19 CAR T-cell infusion. Furthermore, multivariable models including CRS-related cytokines identified associations between higher peak serum concentrations of interleukin-6 and lower day-28 cell counts; in contrast, higher serum concentrations of transforming growth factor-β1 were associated with higher counts. Our findings suggest that patient selection and improved CRS management may improve hematopoietic recovery after CD19 CAR T-cell therapy.
CD19 靶向嵌合抗原受体 (CAR) T 细胞疗法在复发/难治性 B 细胞恶性肿瘤患者中显示出显著疗效;然而,它与细胞因子释放综合征 (CRS)、神经毒性和造血恢复受损等毒性有关。后者与需要延长生长因子或输血支持的高级别细胞减少症相关,可能导致感染或出血等额外并发症。迄今为止,与血液毒性相关的独立因素尚未得到很好的描述。为了解决这一缺陷,我们回顾性分析了在 1 期/2 期临床试验(https://clinicaltrials.gov;NCT01865617)中接受定义组成的 CD19 CAR T 细胞治疗的 173 名患者,主要终点是 CAR T 细胞输注后第 28 天的绝对中性粒细胞计数和血小板计数。我们观察到输注后第 28 天中性粒细胞和血小板恢复的累积发生率分别为 81%和 75%。在很大一部分患者中观察到血液毒性,最后一次随访时仍有 9%的患者持续中性粒细胞减少症和 14%的血小板减少症。使用无偏最小绝对收缩选择器和操作员回归分析进行高维建模,并考虑患者、疾病和治疗相关变量,我们发现 CRS 严重程度增加是血小板计数降低的独立预测因子,而预淋巴细胞减少前血小板计数降低是 CD19 CAR T 细胞输注后中性粒细胞和血小板计数降低的独立预测因子。此外,包括 CRS 相关细胞因子在内的多变量模型确定了白细胞介素-6 血清峰浓度较高与第 28 天细胞计数较低之间的关联;相反,转化生长因子-β1 血清浓度较高与计数较高相关。我们的研究结果表明,患者选择和改进 CRS 管理可能会改善 CD19 CAR T 细胞治疗后的造血恢复。