Department of Medicine III, University Hospital, Ludwig Maximilian University (LMU) Munich, Munich, Germany.
Laboratory for Translational Cancer Immunology, LMU Gene Center, Munich, Germany.
Blood. 2021 Dec 16;138(24):2499-2513. doi: 10.1182/blood.2020010543.
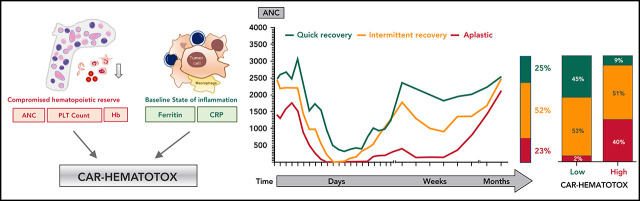
Hematotoxicity represents a frequent chimeric antigen receptor (CAR) T-cell-related adverse event and remains poorly understood. In this multicenter analysis, we studied patterns of hematopoietic reconstitution and evaluated potential predictive markers in 258 patients receiving axicabtagene ciloleucel (axi-cel) or tisagenlecleucel (tisa-cel) for relapsed/refractory large B-cell lymphoma. We observed profound (absolute neutrophil count [ANC] <100 cells per µL) neutropenia in 72% of patients and prolonged (21 days or longer) neutropenia in 64% of patients. The median duration of severe neutropenia (ANC < 500 cells per µL) was 9 days. We aimed to identify predictive biomarkers of hematotoxicity using the duration of severe neutropenia until day +60 as the primary end point. In the training cohort (n = 58), we observed a significant correlation with baseline thrombocytopenia (r = -0.43; P = .001) and hyperferritinemia (r = 0.54; P < .0001) on univariate and multivariate analysis. Incidence and severity of cytokine-release syndrome, immune effector cell-associated neurotoxicity syndrome, and peak cytokine levels were not associated with the primary end point. We created the CAR-HEMATOTOX model, which included markers associated with hematopoietic reserve (eg, platelet count, hemoglobin, and ANC) and baseline inflammation (eg, C-reactive protein and ferritin). This model was validated in independent cohorts, one from Europe (n = 91) and one from the United States (n = 109) and discriminated patients with severe neutropenia ≥14 days to <14 days (pooled validation: area under the curve, 0.89; sensitivity, 89%; specificity, 68%). A high CAR-HEMATOTOX score resulted in a longer duration of neutropenia (12 vs 5.5 days; P < .001) and a higher incidence of severe thrombocytopenia (87% vs 34%; P < .001) and anemia (96% vs 40%; P < .001). The score implicates bone marrow reserve and inflammation prior to CAR T-cell therapy as key features associated with delayed cytopenia and will be useful for risk-adapted management of hematotoxicity.
血液毒性是嵌合抗原受体 (CAR) T 细胞相关的常见不良事件,但仍知之甚少。在这项多中心分析中,我们研究了 258 例接受 axicabtagene ciloleucel (axi-cel) 或 tisagenlecleucel (tisa-cel) 治疗复发/难治性大 B 细胞淋巴瘤患者的造血重建模式,并评估了潜在的预测标志物。我们观察到 72%的患者出现严重中性粒细胞减少症 (绝对中性粒细胞计数 [ANC] <100 个/μL),64%的患者出现中性粒细胞减少症持续时间延长 (21 天或更长时间)。严重中性粒细胞减少症 (ANC < 500 个/μL) 的中位持续时间为 9 天。我们旨在使用严重中性粒细胞减少症持续时间至第 +60 天作为主要终点,确定血液毒性的预测生物标志物。在训练队列 (n = 58) 中,我们观察到基线血小板减少症 (r = -0.43;P =.001) 和高血铁蛋白血症 (r = 0.54;P <.0001) 与单变量和多变量分析相关。细胞因子释放综合征、免疫效应细胞相关神经毒性综合征的发生率和严重程度以及峰值细胞因子水平与主要终点无关。我们创建了 CAR-HEMATOTOX 模型,该模型包括与造血储备相关的标志物 (例如血小板计数、血红蛋白和 ANC) 和基线炎症标志物 (例如 C 反应蛋白和铁蛋白)。该模型在独立队列中得到验证,一个来自欧洲 (n = 91),另一个来自美国 (n = 109),并区分了严重中性粒细胞减少症持续时间≥14 天和 <14 天的患者 (合并验证:曲线下面积,0.89;敏感性,89%;特异性,68%)。高 CAR-HEMATOTOX 评分导致中性粒细胞减少症持续时间更长 (12 天 vs 5.5 天;P <.001),严重血小板减少症发生率更高 (87% vs 34%;P <.001) 和贫血发生率更高 (96% vs 40%;P <.001)。该评分提示 CAR T 细胞治疗前骨髓储备和炎症是与延迟细胞减少相关的关键特征,将有助于血液毒性的风险适应性管理。