Agenzia Italiana del Farmaco, Rome, Italy.
Cardiovascular Center, University Hospital and Health Services of Trieste, Trieste, Italy.
Sci Rep. 2021 Oct 19;11(1):20689. doi: 10.1038/s41598-021-99818-4.
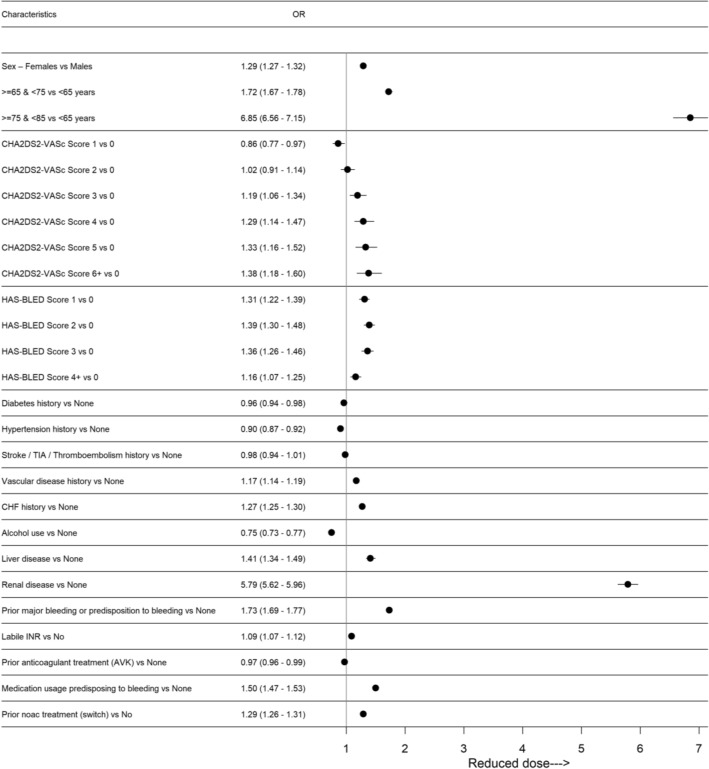
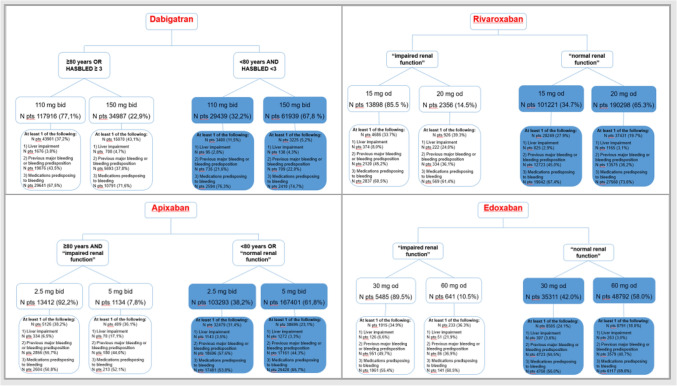
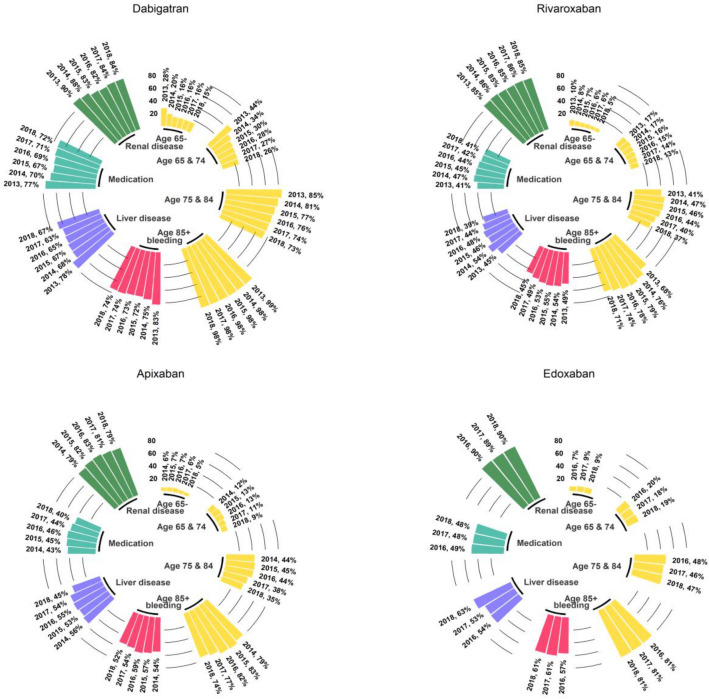
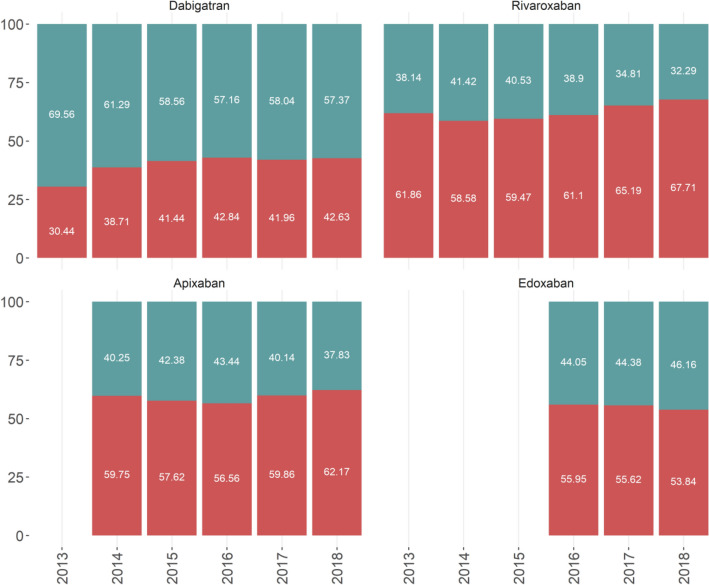
This study aims to provide real-world data about starting-dose of NOACs and dose-adjustment in patients with atrial fibrillation (AF). In fact, even if new oral anticoagulation agents (NOACs) have a predictable effect without need for regular monitoring, dose-adjustments should be performed according to the summary of product information and international guidelines. We employed the Italian Medicines Agency monitoring registries comprising data on a nationwide cohort of patients with AF treated with NOACs from 2013 to 2018. Logistic regression analysis was used to evaluate the determinants of dosage choice. During the reference period, treatment was commenced for 866,539 patients. Forty-five percent of the first prescriptions were dispensed at a reduced dose (dabigatran 60.3%, edoxaban 45.2%, apixaban 40.9%, rivaroxaban 37.4%). The prescription of reduced dose was associated with older age, renal disease, bleeding risk and the concomitant use of drugs predisposing to bleeding, but not with CHADS-VASc and HAS-BLED. A relative reduction of the proportion of patients treated with low dosages was evident overtime for dabigatran and rivaroxaban; whereas prescription of low dose apixaban and edoxaban increased progressively among elderly patients. Evidence based on real-world data shows a high frequency of low dose prescriptions of NOACs in AF patients. Except for older age, renal disease, bleeding risk and the concomitant use of drugs predisposing to bleeding, other factors that may determine the choice of reduced dose could not be ascertained. There may be potential under-treatment of AF patients, but further evaluation is warranted.
本研究旨在提供有关非维生素 K 拮抗剂口服抗凝剂(NOACs)起始剂量和剂量调整的真实世界数据。实际上,即使新型口服抗凝剂(NOACs)具有可预测的作用,无需常规监测,仍应根据产品信息摘要和国际指南进行剂量调整。我们使用了意大利药品管理局监测登记处的数据,这些数据包括 2013 年至 2018 年期间使用 NOACs 治疗的房颤患者的全国性队列数据。使用逻辑回归分析评估了剂量选择的决定因素。在参考期内,有 866539 名患者开始接受治疗。首次处方中有 45%开的是低剂量(达比加群 60.3%、依度沙班 45.2%、阿哌沙班 40.9%、利伐沙班 37.4%)。开低剂量处方与年龄较大、肾脏疾病、出血风险以及同时使用易引起出血的药物有关,但与 CHADS-VASc 和 HAS-BLED 无关。达比加群和利伐沙班的患者接受低剂量治疗的比例随着时间的推移逐渐降低;而低剂量阿哌沙班和依度沙班的处方在老年患者中逐渐增加。基于真实世界数据的证据表明,房颤患者中低剂量 NOACs 的处方频率很高。除了年龄较大、肾脏疾病、出血风险和同时使用易引起出血的药物外,其他可能决定降低剂量选择的因素尚不清楚。可能存在房颤患者治疗不足的情况,但需要进一步评估。