Erasmus MC Transplant Institute, Division HPB and Transplant Surgery, Department of Surgery, Erasmus MC, University Medical Center, Rotterdam, The Netherlands.
Erasmus MC Transplant Institute, Division of Nephrology, Department of Internal Medicine, Erasmus MC, University Medical Center, Rotterdam, The Netherlands.
Clin Transplant. 2022 Jan;36(1):e14515. doi: 10.1111/ctr.14515. Epub 2021 Nov 9.
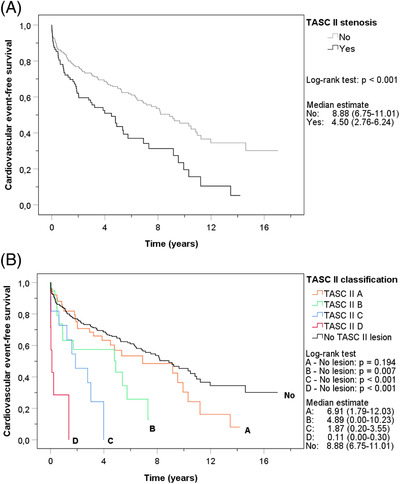
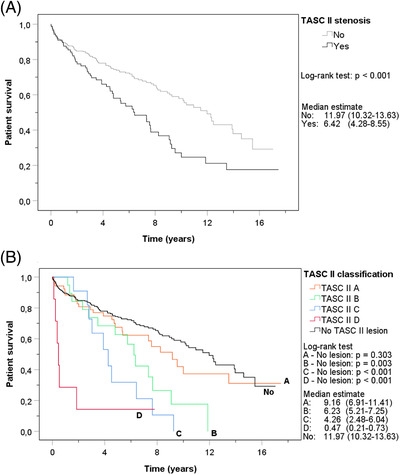
Prediction of the risk of cardiovascular events (CVE's) is important to optimize outcomes after kidney transplantation. Aortoiliac stenosis is frequently observed during pre-transplant screening. We hypothesized that these patients are at higher risk of post-transplant CVE's due to the joint underlying atherosclerotic disease. Therefore, we aimed to assess whether aortoiliac stenosis was associated with post-transplant CVE's. This retrospective, single-center cohort study included adult kidney transplant recipients, transplanted between 2000 and 2016, with contrast-enhanced imaging available. Aortoiliac stenosis was classified according to the Trans-Atlantic Inter-Society Consensus (TASC) II classification and was defined as significant in case of ≥50% lumen narrowing. The primary outcome was CVE-free survival. Eighty-nine of 367 patients had significant aortoiliac stenosis and were found to have worse CVE-free survival (median CVE-free survival: stenosis 4.5 years (95% confidence interval (CI) 2.8-6.2), controls 8.9 years (95% CI 6.8-11.0); log-rank test P < .001). TASC II C and D lesions were independent risk factors for a post-transplant CVE with a hazard ratio of 2.15 (95% CI 1.05-4.38) and 6.56 (95% CI 2.74-15.70), respectively. Thus, kidney transplant recipients with TASC II C and D aortoiliac stenosis require extensive cardiovascular risk management pre-, peri,- and post-transplantation.
预测心血管事件 (CVE) 的风险对于优化肾移植后的结果非常重要。在移植前筛查期间,常观察到主髂动脉狭窄。我们假设这些患者由于共同的动脉粥样硬化疾病,在移植后发生 CVE 的风险更高。因此,我们旨在评估主髂动脉狭窄是否与移植后 CVE 相关。这项回顾性、单中心队列研究纳入了 2000 年至 2016 年间接受过增强成像检查的成年肾移植受者。根据跨大西洋内科学会共识 (TASC) II 分类对主髂动脉狭窄进行分类,如果管腔狭窄≥50%,则定义为显著狭窄。主要结局是 CVE 无事件生存率。在 367 名患者中,有 89 名患有显著的主髂动脉狭窄,发现他们的 CVE 无事件生存率较差(中位 CVE 无事件生存率:狭窄组 4.5 年(95%CI 2.8-6.2),对照组 8.9 年(95%CI 6.8-11.0);对数秩检验 P<.001)。TASC II C 和 D 病变是移植后 CVE 的独立危险因素,风险比分别为 2.15(95%CI 1.05-4.38)和 6.56(95%CI 2.74-15.70)。因此,TASC II C 和 D 型主髂动脉狭窄的肾移植受者需要在移植前、移植期间和移植后进行广泛的心血管风险管理。