Unit of Medical Oncology 2, Azienda Ospedaliero-Universitaria Pisana, Pisa, Italy; Department of Translational Research and New Technology in Medicine and Surgery, University of Pisa, Pisa, Italy.
Service of Pneumo-Oncology, Unit of Pneumology, Azienda Ospedaliero-Universitaria Pisana, Pisa, Italy; Department of Surgical, Medical and Molecular Pathology and Critical Care Medicine, University of Pisa, Pisa, Italy.
ESMO Open. 2021 Dec;6(6):100293. doi: 10.1016/j.esmoop.2021.100293. Epub 2021 Oct 22.
TRIBE and TRIBE-2 studies demonstrated higher benefit from FOLFOXIRI (fluorouracil, leucovorin, oxaliplatin, and irinotecan)/bevacizumab compared with FOLFIRI (fluorouracil, leucovorin, and irinotecan) or FOLFOX/bevacizumab as an upfront option for metastatic colorectal cancer patients, with more toxicities. We focused on the incidence and longitudinal dynamics of neutropenia and febrile neutropenia (FN) in the two studies, to evaluate their clinical relevance, the magnitude of impact of FOLFOXIRI/bevacizumab, and the role of risk factors in predicting their occurrence.
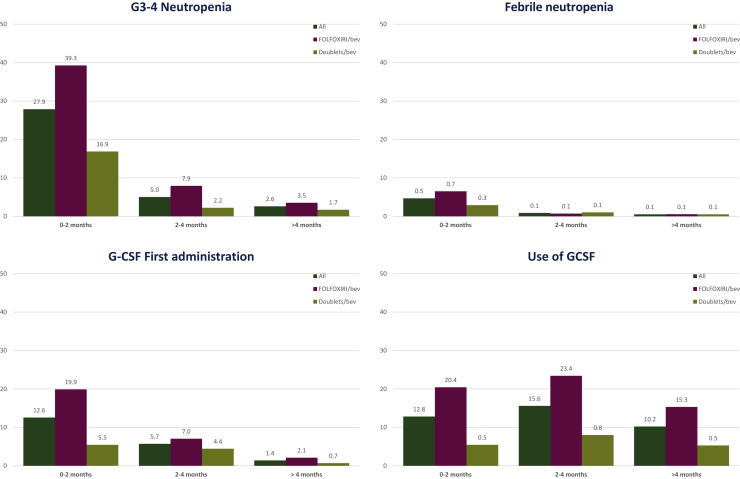
The overall incidence of grade 3-4 (G3-4) neutropenia and FN, the time to their onset, the use of granulocyte colony-stimulating factor, and the association with risk factors were evaluated in the overall population and according to treatment arm. FN episodes were assessed by Multinational Association for Supportive Care in Cancer (MASCC) score.
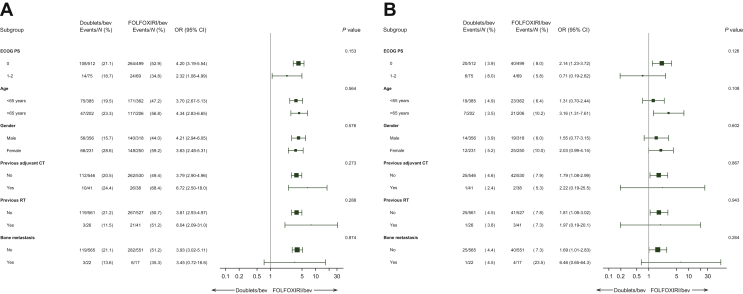
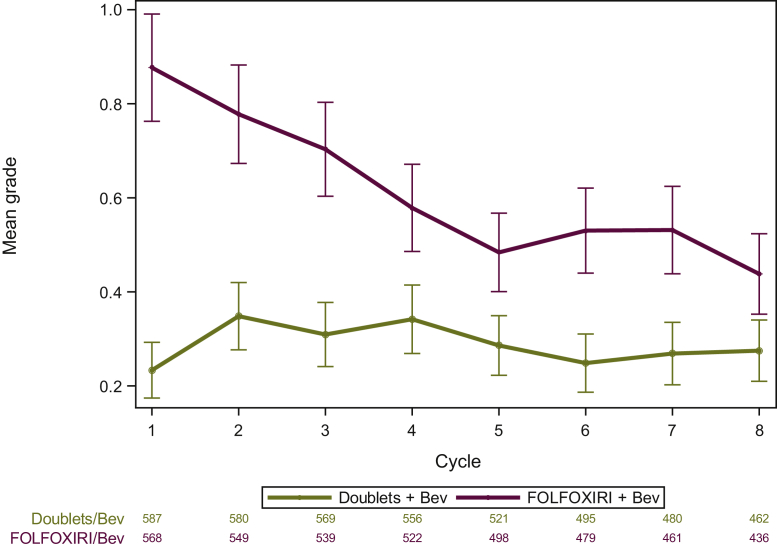
Among 1155 patients, 568 (49%) received FOLFOXIRI/bevacizumab. Overall, 410 (35%) experienced G3-4 neutropenia and 70 (6%) FN, 21 (2%) at high risk. FOLFOXIRI/bevacizumab was associated with higher incidence of neutropenia (51% versus 21%, P < 0.001), FN (8% versus 4%, P = 0.02), and high-risk FN [18 (3%) versus 3 (1%), P = 0.015]. No related deaths were observed. The first episode of G3-4 neutropenia and FN occurred mainly in the first 2 months in both arms. Longitudinal analysis showed different patterns of evolution over cycles between the arms (P < 0.001) G3-4 neutropenia being more frequent in the first cycles with FOLFOXIRI/bevacizumab. Older patients (P = 0.01) and females (P < 0.001) had a significantly higher risk of G3-4 neutropenia. No significant interaction effect between arm and analysed risk factors in terms of risk of G3-4 neutropenia or FN was observed. The incidence of FN among older females receiving FOLFOXIRI/bevacizumab was 12%. Neither G3-4 neutropenia nor FN impaired efficacy in terms of overall response rate, progression-free survival, and overall survival.
FOLFOXIRI/bevacizumab has a higher risk of G3-4 neutropenia and FN than doublets/bevacizumab. FN occurred in <10% of patients, mostly as low-risk episodes. A closer monitoring during the first 2 months is recommended; prophylactic use of granulocyte colony-stimulating factor may be considered for older females.
TRIBE 和 TRIBE-2 研究表明,与 FOLFIRI(氟尿嘧啶、亚叶酸钙和伊立替康)或 FOLFOX(氟尿嘧啶、亚叶酸钙和奥沙利铂)联合贝伐珠单抗相比,FOLFOXIRI(氟尿嘧啶、亚叶酸钙、奥沙利铂和伊立替康)联合贝伐珠单抗作为转移性结直肠癌患者的一线治疗方案具有更高的获益,但其毒性也更大。我们主要关注两项研究中性粒细胞减少症和发热性中性粒细胞减少症(FN)的发生率和纵向动态变化,以评估其临床意义、FOLFOXIRI/贝伐珠单抗的影响程度,以及预测其发生的危险因素的作用。
在总体人群和治疗组中,评估了所有患者中 3-4 级(G3-4)中性粒细胞减少症和 FN 的总发生率、发生时间、粒细胞集落刺激因子的使用情况,以及与危险因素的关系。采用多国支持治疗癌症协会(MASCC)评分评估 FN 发作情况。
在 1155 例患者中,568 例(49%)接受了 FOLFOXIRI/贝伐珠单抗治疗。总体而言,410 例(35%)出现 G3-4 中性粒细胞减少症,70 例(6%)发生 FN,21 例(2%)为高危 FN。与 FOLFOXIRI/贝伐珠单抗相比,中性粒细胞减少症(51%比 21%,P<0.001)、FN(8%比 4%,P=0.02)和高危 FN[18 例(3%)比 3 例(1%),P=0.015]的发生率更高。未观察到与治疗相关的死亡。两组中首次发生 G3-4 中性粒细胞减少症和 FN 主要发生在治疗的前 2 个月。纵向分析显示,两组之间在各周期中中性粒细胞减少症和 FN 的演变模式不同(P<0.001),FOLFOXIRI/贝伐珠单抗治疗组的第 1 个周期中更常发生 G3-4 中性粒细胞减少症。老年患者(P=0.01)和女性(P<0.001)发生 G3-4 中性粒细胞减少症的风险显著增加。在 G3-4 中性粒细胞减少症或 FN 的风险方面,未观察到臂间和分析的危险因素之间存在显著的交互作用。接受 FOLFOXIRI/贝伐珠单抗治疗的老年女性 FN 的发生率为 12%。G3-4 中性粒细胞减少症和 FN 均未影响总体缓解率、无进展生存期和总生存期的疗效。
与 FOLFOXIRI 联合贝伐珠单抗相比,FOLFOXIRI 联合贝伐珠单抗发生 G3-4 中性粒细胞减少症和 FN 的风险更高。FN 发生在<10%的患者中,大多为低危发作。建议在前 2 个月内密切监测;对于老年女性,可考虑预防性使用粒细胞集落刺激因子。