Division of Diabetes, Endocrinology and Metabolic Diseases, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, MD
Division of Cancer Prevention, National Cancer Institute, National Institutes of Health, Rockville, MD.
Diabetes Care. 2021 Dec;44(12):2775-2782. doi: 10.2337/dc21-1046. Epub 2021 Oct 25.
To determine whether metformin or lifestyle modification can lower rates of all-cause and cause-specific mortality in the Diabetes Prevention Program and Diabetes Prevention Program Outcomes Study.
From 1996 to 1999, 3,234 adults at high risk for type 2 diabetes were randomized to an intensive lifestyle intervention, masked metformin, or placebo. Placebo and lifestyle interventions stopped in 2001, and a modified lifestyle program was offered to everyone, but unmasked study metformin continued in those originally randomized. Causes of deaths through 31 December 2018 were adjudicated by blinded reviews. All-cause and cause-specific mortality hazard ratios (HRs) were estimated from Cox proportional hazards regression models and Fine-Gray models, respectively.
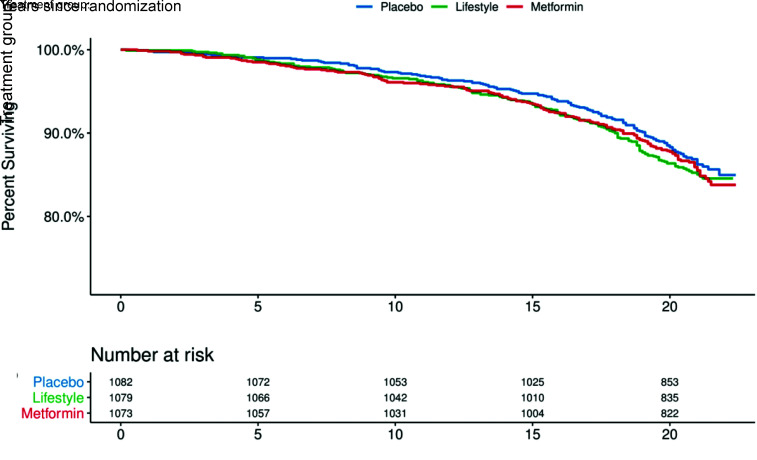
Over a median of 21 years (interquartile range 20-21), 453 participants died. Cancer was the leading cause of death ( = 170), followed by cardiovascular disease ( = 131). Compared with placebo, metformin did not influence mortality from all causes (HR 0.99 [95% CI 0.79, 1.25]), cancer (HR 1.04 [95% CI 0.72, 1.52]), or cardiovascular disease (HR 1.08 [95% CI 0.70, 1.66]). Similarly, lifestyle modification did not impact all-cause (HR 1.02 [95% CI 0.81, 1.28]), cancer (HR 1.07 [95% CI 0.74, 1.55]), or cardiovascular disease (HR 1.18 [95% CI 0.77, 1.81]) mortality. Analyses adjusted for diabetes status and duration, BMI, cumulative glycemic exposure, and cardiovascular risks yielded results similar to those for all-cause mortality.
Cancer was the leading cause of mortality among adults at high risk for type 2 diabetes. Although metformin and lifestyle modification prevented diabetes, neither strategy reduced all-cause, cancer, or cardiovascular mortality rates.
确定二甲双胍或生活方式改变能否降低糖尿病预防计划(Diabetes Prevention Program,DPP)和糖尿病预防计划结局研究(Diabetes Prevention Program Outcomes Study,DPPOS)中全因和特定原因死亡率。
1996 年至 1999 年,3234 名有 2 型糖尿病高危因素的成年人被随机分为强化生活方式干预组、二甲双胍组和安慰剂组。2001 年停止了安慰剂和生活方式干预,向所有人提供了改良的生活方式方案,但原随机分组的未设盲研究二甲双胍继续进行。通过盲法评审确定截至 2018 年 12 月 31 日的死亡原因。使用 Cox 比例风险回归模型和 Fine-Gray 模型分别估计全因和特定原因死亡率的风险比(hazard ratio,HR)。
中位随访时间 21 年(四分位距 20-21 年),453 名参与者死亡。癌症是主要死亡原因(n = 170),其次是心血管疾病(n = 131)。与安慰剂相比,二甲双胍对全因死亡率(HR 0.99 [95%CI 0.79,1.25])、癌症死亡率(HR 1.04 [95%CI 0.72,1.52])或心血管疾病死亡率(HR 1.08 [95%CI 0.70,1.66])均无影响。同样,生活方式改变对全因死亡率(HR 1.02 [95%CI 0.81,1.28])、癌症死亡率(HR 1.07 [95%CI 0.74,1.55])或心血管疾病死亡率(HR 1.18 [95%CI 0.77,1.81])也无影响。对糖尿病状态和病程、BMI、累积血糖暴露和心血管风险进行调整后的分析结果与全因死亡率的分析结果相似。
癌症是 2 型糖尿病高危人群死亡的主要原因。虽然二甲双胍和生活方式改变预防了糖尿病,但这两种策略都没有降低全因、癌症或心血管疾病的死亡率。