Unit of Neurosurgery, Department of Neurosciences, Hospital A. Manzoni, 23900 Lecco, Italy.
Unit of Neurosurgery, Department of Clinical, Surgical, Diagnostic and Pediatric Sciences, University of Pavia, 27100 Pavia, Italy.
Tomography. 2021 Oct 5;7(4):523-532. doi: 10.3390/tomography7040045.
The simultaneous presence of multiple foci of high-grade glioma is a rare condition with a poor prognosis. By definition, if an anatomical connection through white matter bundles cannot be hypothesized, multiple lesions are defined as multicentric glioma (MC); on the other hand, when this connection exists, it is better defined as multifocal glioma (MF). Whether surgery can be advantageous for these patients has not been established yet. The aim of our study was to critically review our experience and to compare it to the existing literature.
Retrospective analysis of patients operated on for MC HGG in two Italian institutions was performed. Distinction between MC and MF was achieved through revision of MR FLAIR images. Clinical and radiological preoperative and postoperative data were analyzed through chart revision and phone interviews. The same data were extracted from literature review. Univariate and multivariate analyses were conducted for the literature review only, and the null hypothesis was rejected for a -value ≥ 0.05.
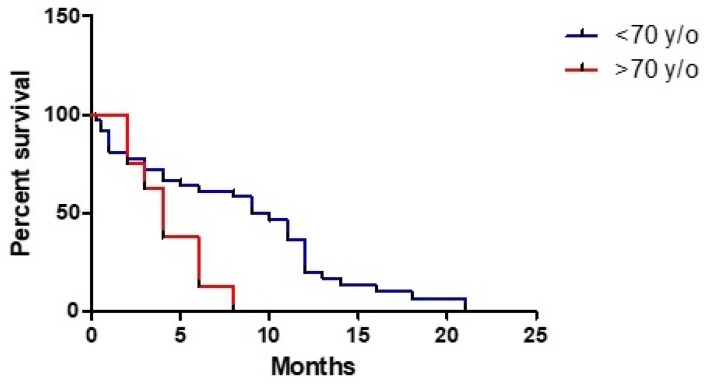
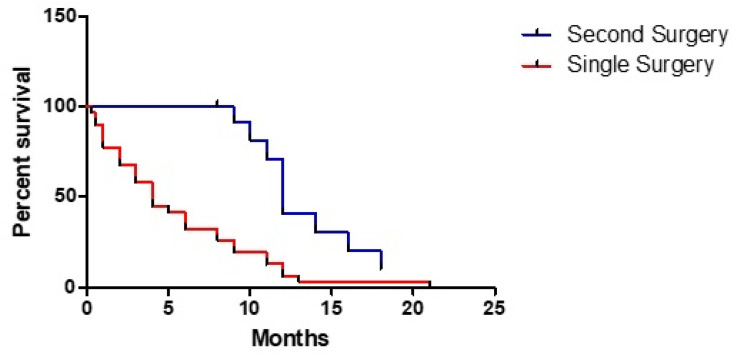
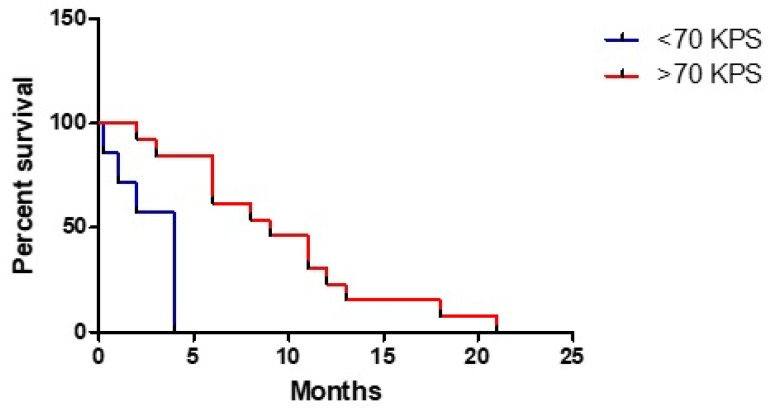
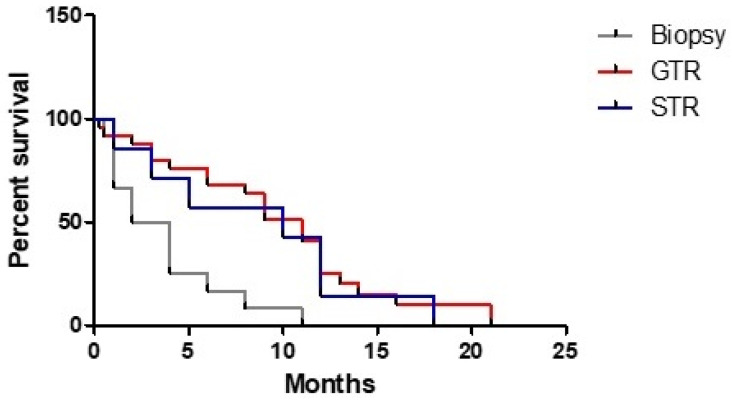
Sixteen patients met the inclusion criteria; male predominance and an average age of 66.5 years were detected. Sensory/motor deficit was the main onset symptom both in clinical study and literature review. A tendency to operate on the largest symptomatic lesion was reported and GTR was reached in the majority of cases. GBM was the histological diagnosis in most part of the patients. OS was 8.7 months in our series compared to 7.5 months from the literature review. Age ≤ 70 years, a postoperative KPS ≥ 70, a GTR/STR, a second surgery and adjuvant treatment were shown to be significantly associated with a better prognosis. Pathological examination revealed that MC HGG did not originate by LGG.
MC gliomas are rare conditions with high malignancy and a poor prognosis. A maximal safe resection should be attempted whenever possible, especially in younger patients with life-threatening large mass.
同时存在多个高级别胶质瘤病灶是一种罕见的预后不良的情况。根据定义,如果不能假设通过白质束的解剖连接,则多个病变被定义为多灶性胶质瘤(MC);另一方面,如果存在这种连接,则更好地定义为多灶性胶质瘤(MF)。是否手术对这些患者有利尚未确定。我们的研究目的是批判性地回顾我们的经验,并将其与现有文献进行比较。
对两家意大利机构接受 MC HGG 手术的患者进行回顾性分析。通过对 MR FLAIR 图像的修订来区分 MC 和 MF。通过图表修订和电话访谈分析临床和影像学术前和术后数据。通过文献回顾提取相同的数据。仅对文献回顾进行单变量和多变量分析,当 - 值≥0.05 时拒绝零假设。
16 名患者符合纳入标准;男性占优势,平均年龄为 66.5 岁。感觉/运动障碍是临床研究和文献回顾中的主要发病症状。报告了倾向于对最大症状性病变进行手术的趋势,并且在大多数情况下达到了 GTR。在大多数患者中,组织学诊断为 GBM。在我们的系列中,OS 为 8.7 个月,而文献回顾为 7.5 个月。年龄≤70 岁、术后 KPS≥70、GTR/STR、二次手术和辅助治疗与更好的预后显著相关。病理检查显示 MC HGG 并非由 LGG 引起。
MC 胶质瘤是罕见的高度恶性和预后不良的疾病。只要可能,应尽可能进行最大安全切除,特别是在有生命威胁的大肿块的年轻患者中。