Department of Diagnostic and Interventional Radiology, Heidelberg University Hospital, Heidelberg, Germany; Diagnostic and Interventional Radiology with Nuclear Medicine, Thoraxklinik at University Hospital Heidelberg, Heidelberg, Germany; Translational Lung Research Center (TLRC), Member of the German Center for Lung Research (DZL), University of Heidelberg, Heidelberg, Germany.
Department of Diagnostic and Interventional Radiology, Heidelberg University Hospital, Heidelberg, Germany; Translational Lung Research Center (TLRC), Member of the German Center for Lung Research (DZL), University of Heidelberg, Heidelberg, Germany.
Eur J Radiol. 2021 Nov;144:110002. doi: 10.1016/j.ejrad.2021.110002. Epub 2021 Oct 19.
To examine the performance of radiologists in differentiating COVID-19 from non-COVID-19 atypical pneumonia and to perform an analysis of CT patterns in a study cohort including viral, fungal and atypical bacterial pathogens.
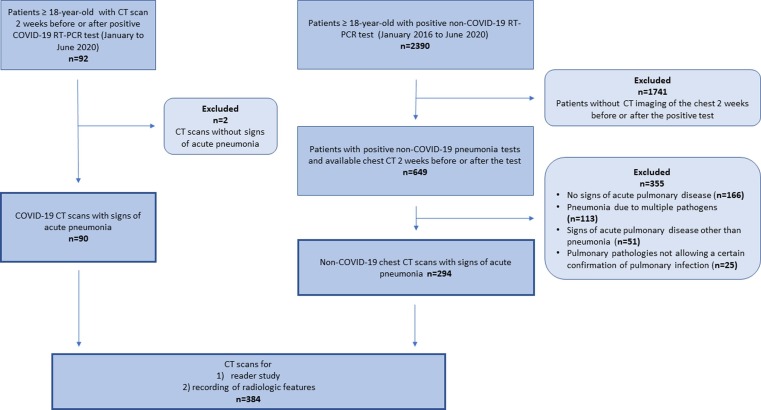
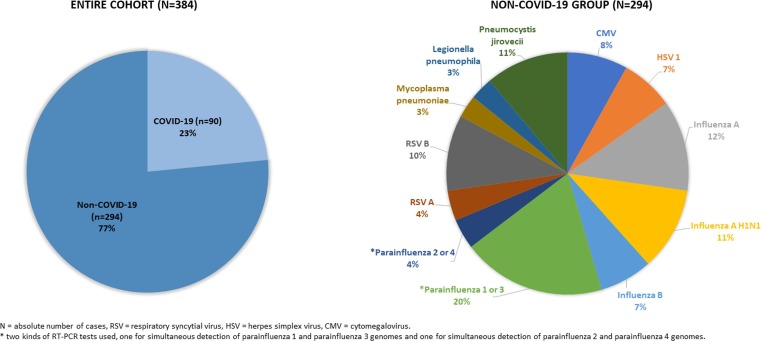
Patients with positive RT-PCR tests for COVID-19 pneumonia (n = 90) and non-COVID-19 atypical pneumonia (n = 294) were retrospectively included. Five radiologists, blinded to the pathogen test results, assessed the CT scans and classified them as COVID-19 or non-COVID-19 pneumonia. For both groups specific CT features were recorded and a multivariate logistic regression model was used to calculate their ability to predict COVID-19 pneumonia.
The radiologists differentiated between COVID-19 and non-COVID-19 pneumonia with an overall accuracy, sensitivity, and specificity of 88% ± 4 (SD), 79% ± 6 (SD), and 90% ± 6 (SD), respectively. The percentage of correct ratings was lower in the early and late stage of COVID-19 pneumonia compared to the progressive and peak stage (68 and 71% vs 85 and 89%). The variables associated with the most increased risk of COVID-19 pneumonia were band like subpleural opacities (OR 5.55, p < 0.001), vascular enlargement (OR 2.63, p = 0.071), and subpleural curvilinear lines (OR 2.52, p = 0.021). Bronchial wall thickening and centrilobular nodules were associated with decreased risk of COVID-19 pneumonia with OR of 0.30 (p = 0.013) and 0.10 (p < 0.001), respectively.
Radiologists can differentiate between COVID-19 and non-COVID-19 atypical pneumonias at chest CT with high overall accuracy, although a lower performance was observed in the early and late stage of COVID 19 pneumonia. Specific CT features might help to make the correct diagnosis.
研究放射科医生在鉴别 COVID-19 与非 COVID-19 非典型性肺炎方面的表现,并对包括病毒、真菌和非典型细菌病原体在内的研究队列中的 CT 模式进行分析。
回顾性纳入经 RT-PCR 检测 COVID-19 肺炎阳性(n=90)和非 COVID-19 非典型性肺炎(n=294)的患者。5 位放射科医生对 CT 扫描结果进行盲法评估,并将其分类为 COVID-19 或非 COVID-19 肺炎。记录两组的特定 CT 特征,并使用多变量逻辑回归模型计算其预测 COVID-19 肺炎的能力。
放射科医生对 COVID-19 和非 COVID-19 肺炎的总体准确率、敏感度和特异度分别为 88%±4(SD)、79%±6(SD)和 90%±6(SD)。与进展期和高峰期相比,COVID-19 肺炎的早期和晚期正确评分较低(分别为 68%和 71%,而 85%和 89%)。与 COVID-19 肺炎风险增加最相关的变量是胸膜下条带状影(OR 5.55,p<0.001)、血管扩张(OR 2.63,p=0.071)和胸膜下线(OR 2.52,p=0.021)。支气管壁增厚和小叶中心结节与 COVID-19 肺炎风险降低相关,OR 分别为 0.30(p=0.013)和 0.10(p<0.001)。
放射科医生可以通过胸部 CT 区分 COVID-19 和非 COVID-19 非典型肺炎,总体准确率较高,但在 COVID-19 肺炎的早期和晚期,表现较低。特定的 CT 特征可能有助于做出正确诊断。