Clinic of Anaesthesiology, Hannover Medical School, Carl-Neuberg-Str.1, 30625, Hannover, Germany.
Clinic of Anaesthesiology, KRH Klinikum Robert Koch, Gehrden, Germany.
BMC Anesthesiol. 2021 Oct 26;21(1):254. doi: 10.1186/s12871-021-01468-6.
Despite well-defined recommendations, prolonged fasting times for clear fluids and solids are still common before elective surgery in adults. Extended fasting times may lead to discomfort, thirst, hunger and physiological dysfunctions. Previous studies have shown that prolonged fasting times are frequently caused by patients being misinformed as well as inadequate implementation of the current guidelines by medical staff. This study aimed to explore how long elective surgery patients fast in a German secondary care hospital before and after the introduction of an educational note for patients and re-training for the medical staff.
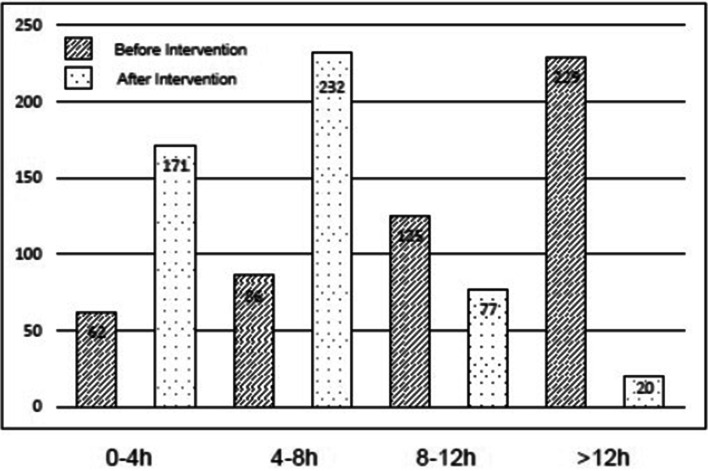
A total of 1002 patients were enrolled in this prospective, non-randomised interventional study. According to the power calculation, in the first part of the study actual fasting times for clear fluids and solids were documented in 502 consecutive patients, verbally instructed as usual regarding the recommended fasting times for clear fluids (2 h) and solids (6 h). Subsequently, we implemented additionally to the verbal instruction a written educational note for the patients, including the recommended fasting times. Furthermore, the medical staff was re-trained regarding the fasting times using emails, newsletters and employee meetings. Thereafter, another 500 patients were included in the study. We hypothesised, that after these quality improvement procedures, actual fasting times for clear fluids and solids would be more accurate on time.
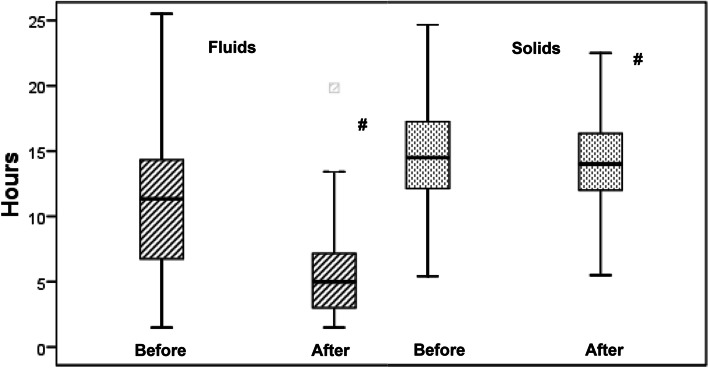
Actual fasting times for clear fluids were in the median 11.3 (interquartile range 6.8-14.3; range 1.5-25.5) h pre-intervention, and were significantly reduced to 5.0 (3.0-7.2; 1.5-19.8) h after the intervention (median difference (95%CI) - 5.5 (- 6.0 to - 5.0) h). The actual fasting times for solids also decreased significantly, but only from 14.5 (12.1-17.2; 5.4-48.0) h to 14.0 (12.0-16.3; 5.4-32.0) h after the interventions (median difference (95%CI) - 0.52 (- 1.0 to - 0.07) h).
The study showed considerably extended actual fasting times in elective adult surgical patients, which were significantly reduced by simple educational/training interventions. However, the actual fasting times still remained considerably longer than defined in recommended guidelines, meaning further process optimisations like obligatory fluid intake in the early morning are necessary to improve patient comfort and safety in future.
German registry of clinical studies (DRKS-ID: DRKS 00020530 , retrospectively registered).
尽管有明确的建议,但成人择期手术前仍普遍存在长时间禁食清水和固体食物的情况。长时间禁食可能导致不适、口渴、饥饿和生理功能紊乱。先前的研究表明,长时间禁食通常是由于患者信息错误以及医务人员未能充分执行当前指南所致。本研究旨在探讨在为患者提供教育说明和重新培训医务人员后,一家德国二级保健医院的择期手术患者术前禁食清水和固体食物的时间。
本前瞻性非随机干预研究共纳入 1002 名患者。根据计算,在研究的第一部分,502 例连续患者接受了实际禁食清水和固体食物的时间记录,口头告知他们推荐的禁食清水(2 小时)和固体(6 小时)时间。随后,我们除口头指导外,还为患者提供了书面教育说明,包括推荐的禁食时间。此外,还通过电子邮件、时事通讯和员工会议重新培训医务人员禁食时间。此后,又有 500 名患者纳入研究。我们假设,在这些质量改进措施后,实际禁食清水和固体食物的时间将更加准确。
术前实际禁食清水时间中位数为 11.3(四分位距 6.8-14.3;范围 1.5-25.5)小时,干预后显著减少至 5.0(3.0-7.2;1.5-19.8)小时(中位数差值(95%CI)-5.5(-6.0 至-5.0)小时)。固体食物的实际禁食时间也显著减少,但仅从 14.5(12.1-17.2;5.4-48.0)小时减少至 14.0(12.0-16.3;5.4-32.0)小时(中位数差值(95%CI)-0.52(-1.0 至-0.07)小时)。
该研究表明,择期手术成年患者的实际禁食时间明显延长,通过简单的教育/培训干预可显著减少。然而,实际禁食时间仍明显长于推荐指南规定的时间,这意味着未来需要进一步优化流程,如清晨强制性补液,以提高患者舒适度和安全性。
德国临床研究注册(DRKS-ID:DRKS00020530,回顾性注册)。