Epidemic Intelligence Service, Centers for Disease Control and Prevention, 1600 Clifton Rd, Atlanta, GA, USA.
Malaria Branch, Division of Parasitic Diseases and Malaria, Center for Global Health, CDC Atlanta, 1600 Clifton Rd, Atlanta, GA, USA.
Malar J. 2021 Oct 26;20(1):422. doi: 10.1186/s12936-021-03956-z.
Integrated community case management of malaria, pneumonia, and diarrhoea can reduce mortality in children under five years (CU5) in resource-poor countries. There is growing interest in expanding malaria community case management (mCCM) to older individuals, but limited empirical evidence exists to guide this expansion. As part of a two-year cluster-randomized trial of mCCM expansion to all ages in southeastern Madagascar, a cross-sectional survey was conducted to assess baseline malaria prevalence and healthcare-seeking behaviours.
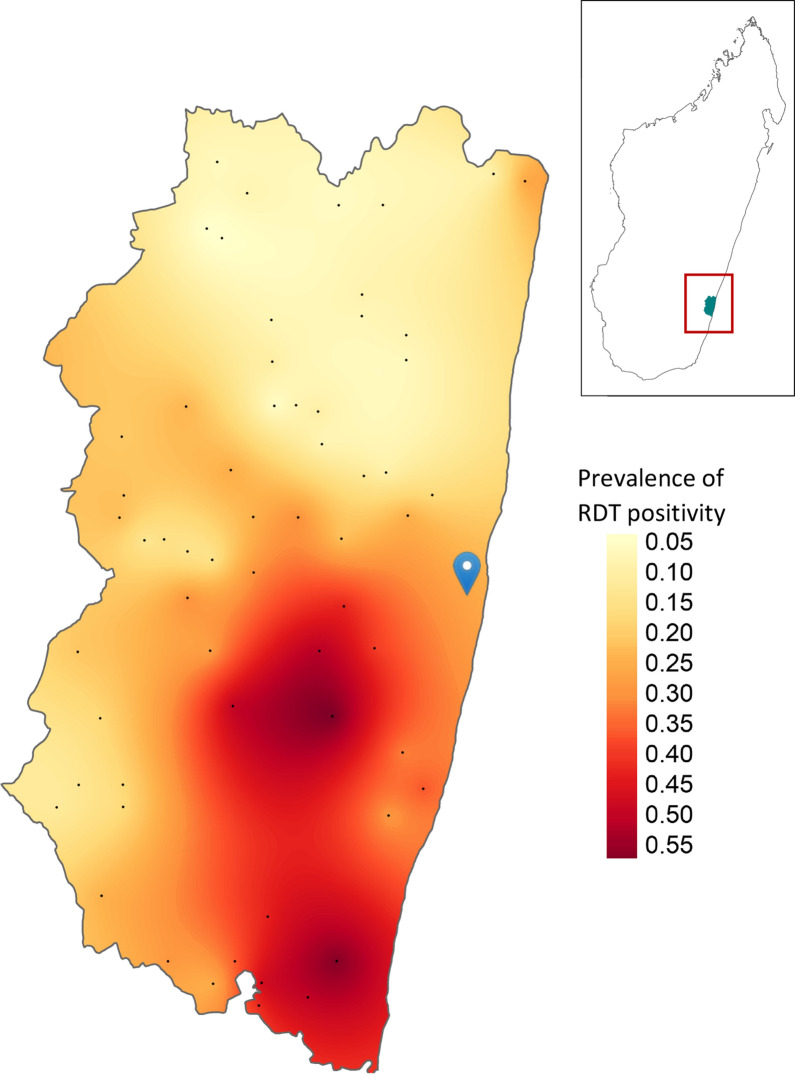
Two enumeration areas (EAs) were randomly chosen from each catchment area of the 30 health facilities (HFs) in Farafangana district designated for the mCCM age expansion trial; 28 households were randomly selected from each EA for the survey. All household members were asked about recent illness and care-seeking, and malaria prevalence was assessed by rapid diagnostic test (RDT) among children < 15 years of age. Weighted population estimates and Rao-Scott chi-squared tests were used to examine illness, care-seeking, malaria case management, and malaria prevalence patterns.
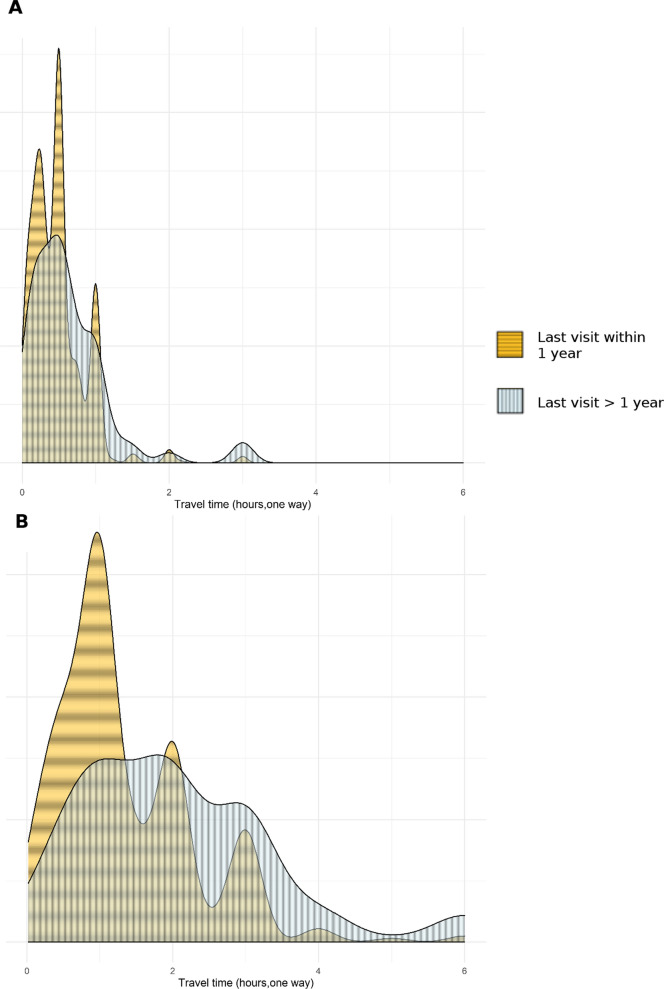
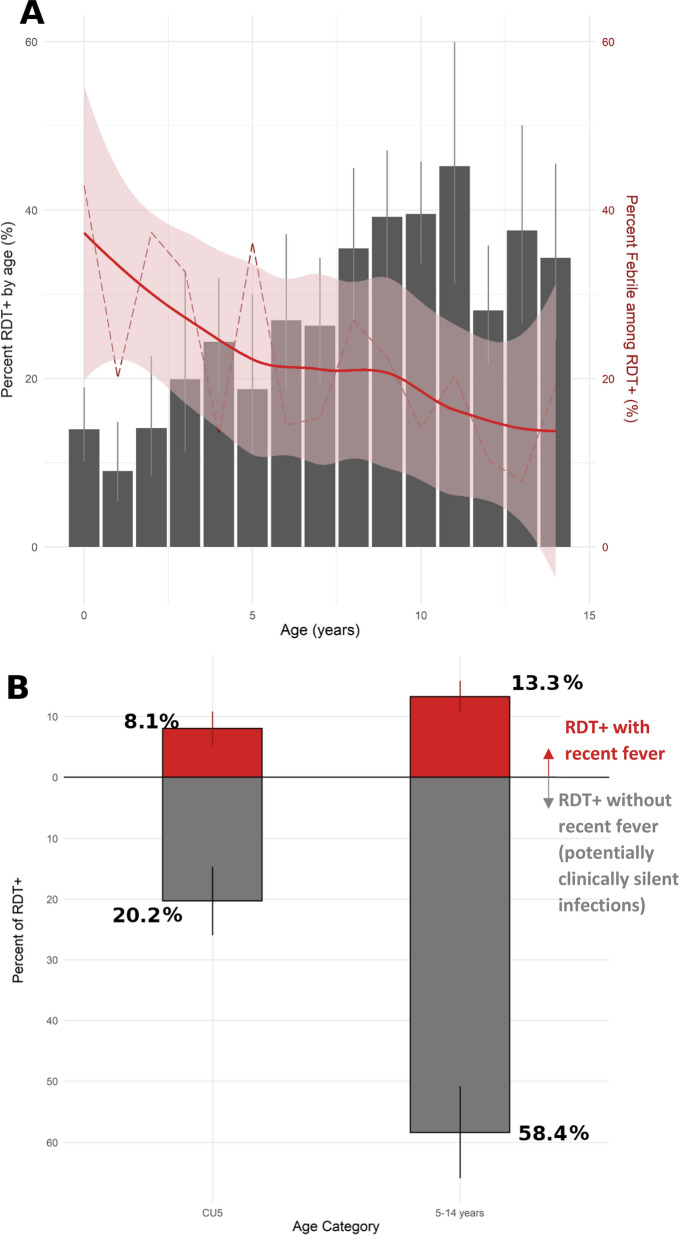
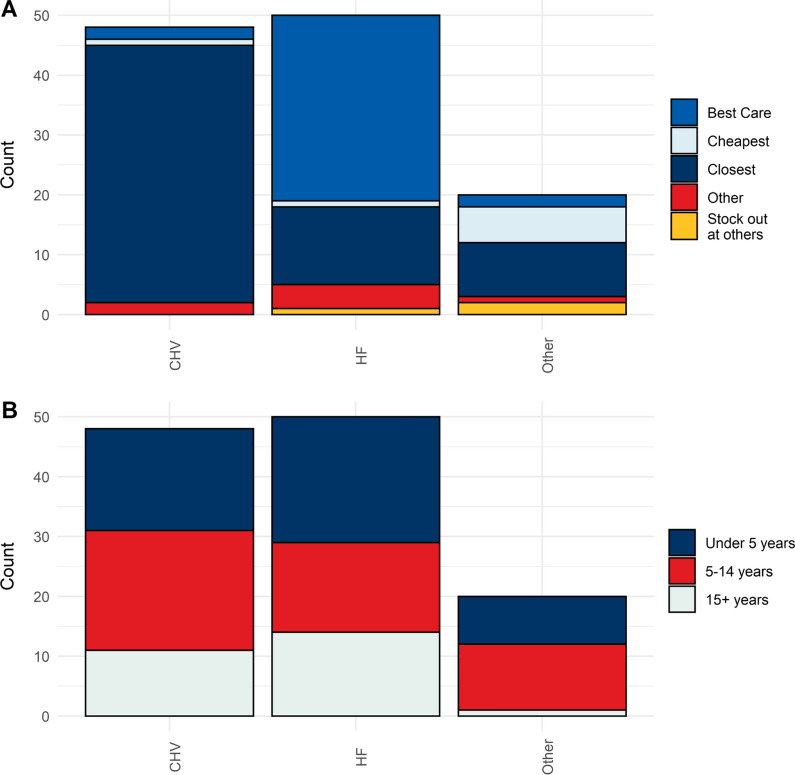
Illness in the two weeks prior to the survey was reported by 459 (6.7%) of 8050 respondents in 334 of 1458 households surveyed. Most individuals noting illness (375/459; 82.3%) reported fever. Of those reporting fever, 28.7% (112/375) sought care; this did not vary by participant age (p = 0.66). Most participants seeking care for fever visited public HFs (48/112, 46.8%), or community healthcare volunteers (CHVs) (40/112, 31.0%). Of those presenting with fever at HFs or to CHVs, 87.0% and 71.0%, respectively, reported being tested for malaria. RDT positivity among 3,316 tested children < 15 years was 25.4% (CI: 21.5-29.4%) and increased with age: 16.9% in CU5 versus 31.8% in 5-14-year-olds (p < 0.0001). Among RDT-positive individuals, 28.4% of CU5 and 18.5% of 5-14-year-olds reported fever in the two weeks prior to survey (p = 0.044).
The higher prevalence of malaria among older individuals coupled with high rates of malaria testing for those who sought care at CHVs suggest that expanding mCCM to older individuals may substantially increase the number of infected individuals with improved access to care, which could have additional favorable effects on malaria transmission.
在资源匮乏的国家,综合社区疟疾、肺炎和腹泻病例管理可降低五岁以下儿童(CU5)的死亡率。人们越来越感兴趣地将疟疾社区病例管理(mCCM)扩大到年龄较大的个体,但指导这一扩展的经验证据有限。作为在马达加斯加东南部将 mCCM 扩大到所有年龄段的为期两年的集群随机试验的一部分,进行了一项横断面调查,以评估疟疾的基线患病率和医疗保健寻求行为。
从法拉凡加纳区 30 个指定用于 mCCM 年龄扩大试验的卫生设施的每个集水区中随机选择两个计数区(EA);从每个 EA 中随机选择 28 户家庭进行调查。询问所有家庭的成员最近是否患病和寻求医疗,对 15 岁以下的儿童进行快速诊断检测(RDT)以评估疟疾患病率。使用加权人口估计和 Rao-Scott 卡方检验来检查疾病、寻求医疗、疟疾病例管理和疟疾流行模式。
在调查前两周内,334 户家庭中的 1458 户中有 8050 名受访者中的 459 名(6.7%)报告患病。大多数报告患病的人(375/459;82.3%)都有发热。在报告发热的人中,28.7%(112/375)寻求医疗;这与参与者的年龄无关(p=0.66)。大多数因发热寻求医疗的人前往公立卫生设施(48/112,46.8%)或社区医疗志愿者(CHVs)(40/112,31.0%)。在前往卫生设施或 CHVs 的发热患者中,分别有 87.0%和 71.0%的人报告接受了疟疾检测。3316 名接受检测的 15 岁以下儿童的 RDT 阳性率为 25.4%(CI:21.5-29.4%),且随年龄增长而增加:CU5 为 16.9%,5-14 岁为 31.8%(p<0.0001)。在 RDT 阳性个体中,CU5 中 28.4%的人和 5-14 岁的人中 18.5%的人在调查前两周内有发热(p=0.044)。
年龄较大的个体中疟疾的更高患病率加上对在 CHVs 寻求医疗的人的疟疾高检测率表明,将 mCCM 扩大到年龄较大的个体可能会大量增加感染人数,同时改善获得医疗的机会,这可能对疟疾传播产生额外的有利影响。