Department of Obstetrics and Gynecology, University Hospital Inselspital Bern, University of Bern, 3010, Bern, Switzerland.
BMC Pregnancy Childbirth. 2021 Oct 27;21(1):728. doi: 10.1186/s12884-021-04209-2.
Healthy women with low risk singleton pregnancies are offered a midwife-led birth model at our department. Exclusion criteria for midwife-led births include a range of abnormalities in medical history and during the course of pregnancy. In case of complications before, during or after labor and birth, an obstetrician is involved. The purpose of this study was 1) to evaluate the frequency of and reasons for secondary obstetrician involvement in planned midwife-led births and 2) to assess the maternal and neonatal outcome.
We analyzed a cohort of planned midwife-led births during a 14 years period (2006-2019). Evaluation included a comparison between midwife-led births with or without secondary obstetrician involvement, regarding maternal characteristics, birth mode, and maternal and neonatal outcome. Statistical analysis was performed by unpaired t-tests and Chi-square tests.
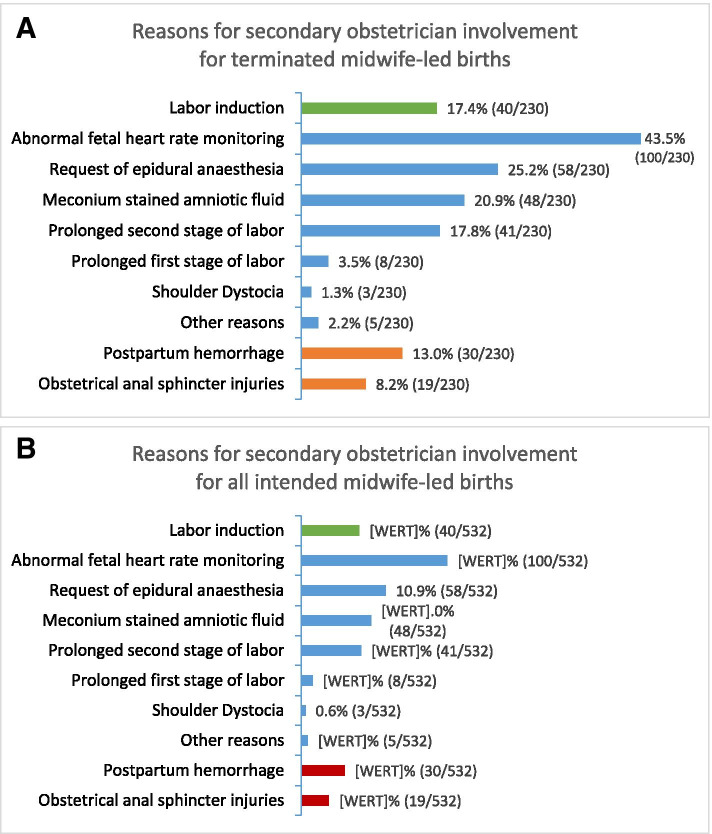
In total, there were 532 intended midwife-led births between 2006 and 2019 (2.6% of all births during this time-period at the department). Among these, 302 (57%) women had spontaneous vaginal births as midwife-led births. In the remaining 230 (43%) births, obstetricians were involved: 62% of women with obstetrician involvement had spontaneous vaginal births, 25% instrumental vaginal births and 13% caesarean sections. Overall, the caesarean section rate was 5.6% in the whole cohort of women with intended midwife-led births. Reasons for obstetrician involvement primarily included necessity for labor induction, abnormal fetal heart rate monitoring, thick meconium-stained amniotic fluid, prolonged first or second stage of labor, desire for epidural analgesia, obstetrical anal sphincter injuries, retention of placenta and postpartum hemorrhage. There was a significantly higher rate of primiparous women in the group with obstetrician involvement. Arterial umbilical cord pH < 7.10 occurred significantly more often in the group with obstetrician involvement, while 5' Apgar score < 7 did not differ significantly. The overall transfer rate of newborns to neonatal intensive care unit was low (1.3%).
A midwife-led birth in our setting is a safe alternative to a primarily obstetrician-led birth, provided that selection criteria are being followed and prompt obstetrician involvement is available in case of abnormal course of labor and birth or postpartum complications.
在我院,低危单胎妊娠的健康女性可选择由助产士主导的分娩模式。由助产士主导分娩的排除标准包括一系列病史和妊娠期间的异常情况。如果在分娩前后出现并发症,将由产科医生介入。本研究的目的是 1)评估计划由助产士主导的分娩中产科医生二次介入的频率和原因,2)评估母婴结局。
我们分析了 14 年间(2006-2019 年)计划由助产士主导的分娩队列。评估包括比较有和没有产科医生二次介入的由助产士主导的分娩,比较产妇特征、分娩方式以及母婴结局。统计分析采用配对 t 检验和卡方检验。
在 2006 年至 2019 年期间,共有 532 名计划由助产士主导的分娩(在此期间该科室所有分娩的 2.6%)。其中,302 名(57%)女性自然阴道分娩作为助产士主导的分娩。在其余 230 名(43%)分娩中,产科医生介入:产科医生介入的女性中,62%自然阴道分娩,25%器械性阴道分娩,13%剖宫产。总体而言,在计划由助产士主导分娩的所有女性中,剖宫产率为 5.6%。产科医生介入的主要原因包括需要引产、胎心监护异常、胎粪污染羊水、第一产程或第二产程延长、需要硬膜外镇痛、产科肛门括约肌损伤、胎盘滞留和产后出血。在有产科医生介入的组中,初产妇的比例明显更高。有产科医生介入的组中,脐动脉 pH 值<7.10 的发生率明显更高,而 5' Apgar 评分<7 无显著差异。新生儿转入新生儿重症监护病房的总体转移率较低(1.3%)。
在我们的环境中,由助产士主导的分娩是一种安全的替代方案,前提是遵循选择标准,并且在分娩过程和产后出现异常或并发症时,能够及时获得产科医生的介入。