Institute of Cardiovascular Science, University College London, London, UK.
Royal Free Hospital, London, UK.
J Cardiovasc Magn Reson. 2021 Oct 28;23(1):118. doi: 10.1186/s12968-021-00817-1.
Exercise intolerance in systemic sclerosis (SSc) is typically attributed to cardiopulmonary limitations. However, problems with skeletal muscle oxygen extraction have not been fully investigated. This study used cardiovascular magnetic resonance (CMR)-augmented cardiopulmonary exercise testing (CMR-CPET) to simultaneously measure oxygen consumption and cardiac output. This allowed calculation of arteriovenous oxygen content gradient, a recognized marker of oxygen extraction. We performed CMR-CPET in 4 groups: systemic sclerosis (SSc); systemic sclerosis-associated pulmonary arterial hypertension (SSc-PAH); non-connective tissue disease pulmonary hypertension (NC-PAH); and healthy controls.
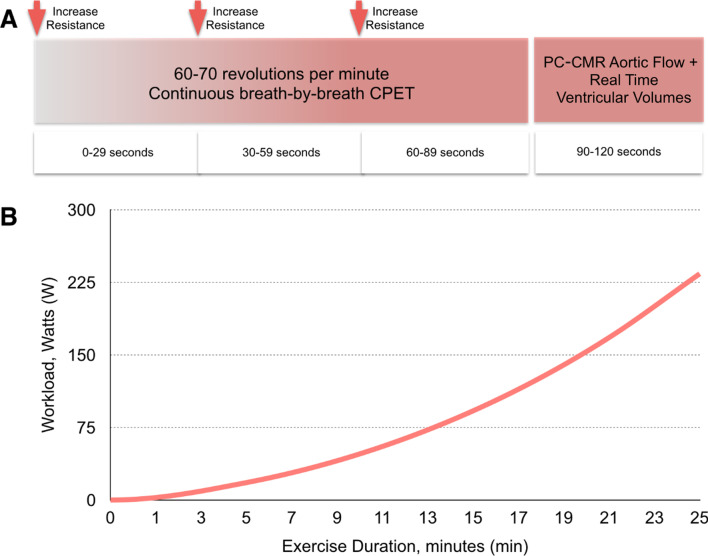
We performed CMR-CPET in 60 subjects (15 in each group) using a supine ergometer following a ramped exercise protocol until exhaustion. Values for oxygen consumption, cardiac output and oxygen content gradient, as well as ventricular volumes, were obtained at rest and peak-exercise for all subjects. In addition, T1 and T2 maps were acquired at rest, and the most recent clinical measures (hemoglobin, lung function, 6-min walk, cardiac and catheterization) were collected.
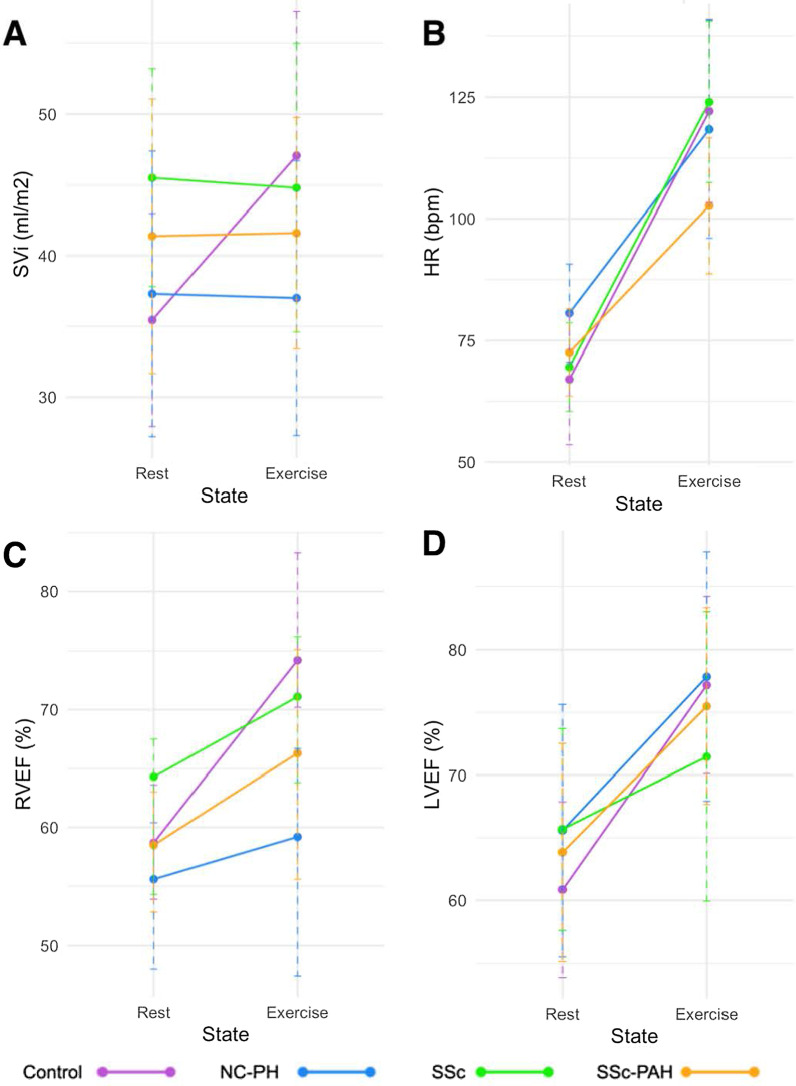
All patient groups had reduced peak oxygen consumption compared to healthy controls (p < 0.022). The SSc and SSc-PAH groups had reduced peak oxygen content gradient compared to healthy controls (p < 0.03). Conversely, the SSc-PAH and NC-PH patients had reduced peak cardiac output compared to healthy controls and SSc patients (p < 0.006). Higher hemoglobin was associated with higher peak oxygen content gradient (p = 0.025) and higher myocardial T1 was associated with lower peak stroke volume (p = 0.011).
Reduced peak oxygen consumption in SSc patients is predominantly driven by reduced oxygen content gradient and in SSc-PAH patients this was amplified by reduced peak cardiac output. Trial registration The study is registered with ClinicalTrials.gov Protocol Registration and Results System (ClinicalTrials.gov ID: 100358).
系统性硬化症(SSc)患者的运动不耐受通常归因于心肺功能受限。然而,骨骼肌氧摄取问题尚未得到充分研究。本研究使用心血管磁共振(CMR)增强心肺运动测试(CMR-CPET)同时测量耗氧量和心输出量。这允许计算动静脉氧含量梯度,这是氧摄取的公认标志物。我们对 4 组患者进行了 CMR-CPET 检查:系统性硬化症(SSc);系统性硬化症相关肺动脉高压(SSc-PAH);非结缔组织疾病性肺动脉高压(NC-PAH);和健康对照组。
我们使用仰卧式测力计在斜坡运动方案下对 60 名受试者(每组 15 名)进行 CMR-CPET,直至力竭。在所有受试者中,在休息和最大运动时获得耗氧量、心输出量和氧含量梯度以及心室容积的值。此外,在休息时采集 T1 和 T2 图,并采集最新的临床指标(血红蛋白、肺功能、6 分钟步行、心脏和导管检查)。
与健康对照组相比,所有患者组的最大耗氧量均降低(p<0.022)。SSc 和 SSc-PAH 组的最大氧含量梯度较健康对照组降低(p<0.03)。相反,SSc-PAH 和 NC-PH 患者的最大心输出量较健康对照组和 SSc 患者降低(p<0.006)。较高的血红蛋白与较高的最大氧含量梯度相关(p=0.025),较高的心肌 T1 与较低的最大心搏量相关(p=0.011)。
SSc 患者的最大耗氧量降低主要由氧含量梯度降低引起,而 SSc-PAH 患者则由最大心输出量降低引起。试验注册本研究在 ClinicalTrials.gov 注册和结果系统(ClinicalTrials.gov ID:100358)中注册。