Medicines Patent Pool, Geneva, Switzerland.
Medicines Patent Pool, Geneva, Switzerland.
Lancet Public Health. 2022 Feb;7(2):e169-e176. doi: 10.1016/S2468-2667(21)00202-4. Epub 2021 Oct 26.
Non-exclusive voluntary licensing that is access-oriented has been suggested as an option to increase access to medicines to address the COVID-19 pandemic. To date, there has been little research on the effect of licensing, mainly focused on economic and supply chain considerations, and not on the benefits in terms of health outcomes. We aimed to study the economic and health effect of voluntary licensing for medicines for HIV and hepatitis C virus (HCV) in low-income and middle-income countries (LMICs).
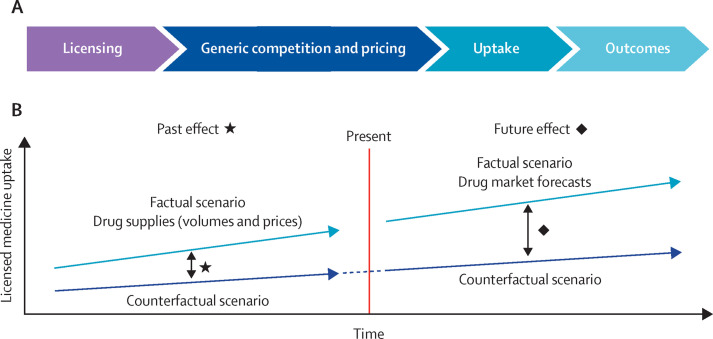
A robust modelling framework was created to examine the difference between scenarios, with (factual) and without (counterfactual) a Medicines Patent Pool (MPP) licence for two medicines, dolutegravir and daclatasvir. Data were obtained from MPP licensees, as well as a large number of external sources. The primary outcomes were the cost savings and health impact between scenarios with and without MPP licences across all LMICs. Through its licences, MPP had access to the volumes and prices of licensed generic products sold in all covered countries on a quarterly basis. These data informed the volumes, prices, and uptake for the past factual scenarios and were the basis for modelling the future factual scenarios. These scenarios were then compared with a set of counterfactual scenarios in the absence of the studied licences.
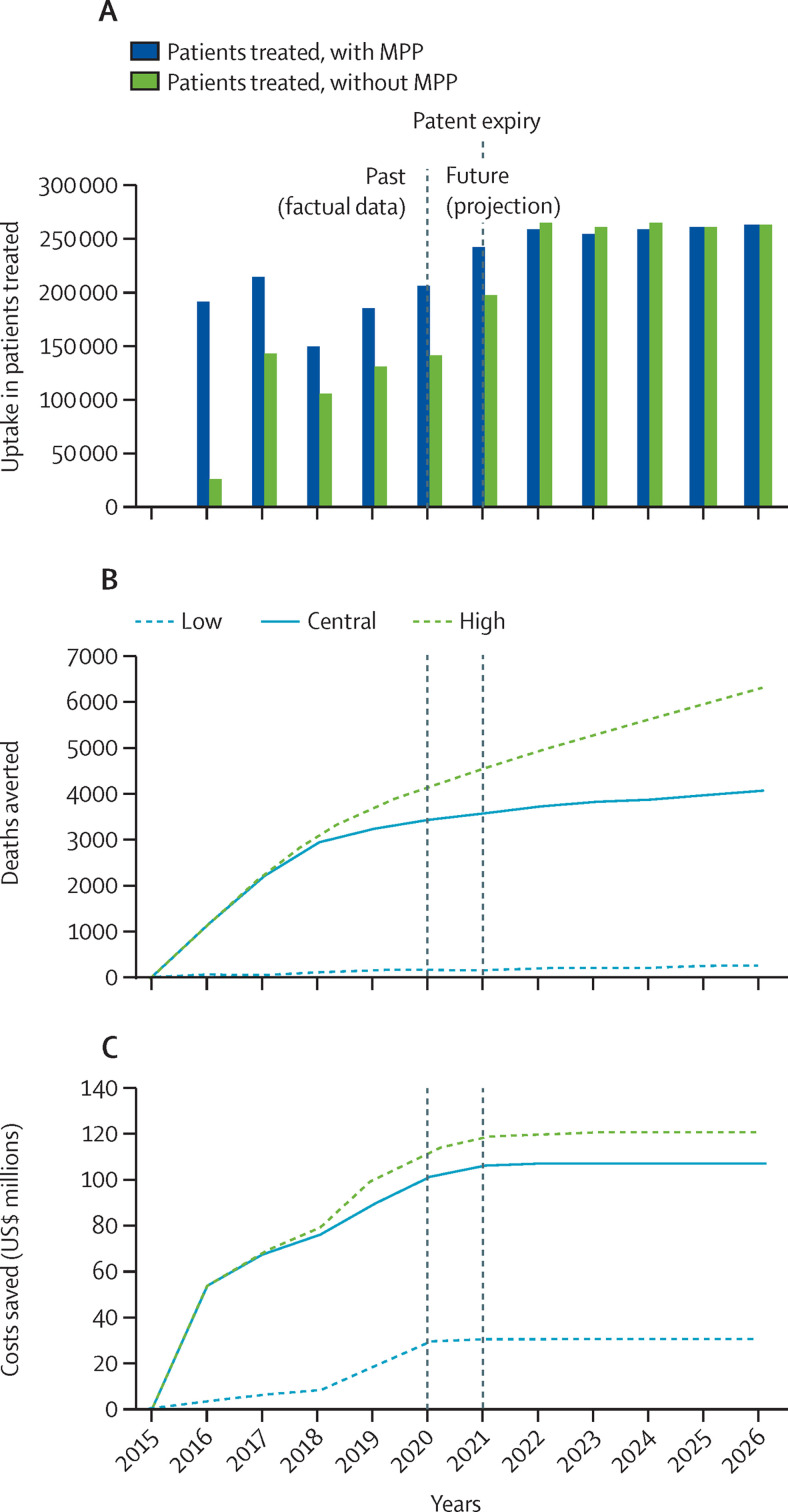
Cumulatively, between 2017 and 2032, the model's central assumptions predicted an additional uptake of 15·494 (range 14·406-15·494) million patient-years of dolutegravir-based HIV treatments, 151 839 (34 575-312 973) deaths averted, and US$3·074 (1·837-5·617) billion saved through the MPP licence compared with the counterfactual scenario. For daclatasvir-based HCV treatments, the cumulative effect from 2015 to 2026 was predicted to be an additional uptake of 428 244 (127 584-636 270) patients treated with daclatasvir, 4070 (225-6323) deaths averted, and $107·593 (30·377-121·284) million saved with the licence compared with the counterfactual scenario.
The chain of effects linking upstream licensing to downstream outcomes can be modelled. Accordingly, credible quantitative estimates of economic and health effects arising from access-oriented voluntary licensing were obtained based on assumptions that early generic competition leads to price reductions that influence procurement decisions and enable the faster and broader uptake of recommended medicines, with beneficial economic and health effects.
Unitaid.
以获取为导向的非独家自愿许可已被提议作为增加药物获取以应对 COVID-19 大流行的一种选择。迄今为止,关于许可的影响的研究很少,主要集中在经济和供应链方面,而不是在健康结果方面的收益。我们旨在研究在中低收入国家(LMICs)中针对艾滋病毒和丙型肝炎病毒(HCV)药物的自愿许可的经济和健康影响。
创建了一个稳健的建模框架来研究有(实际)和没有(假设)药品专利池(MPP)许可情况下两种药物(多替拉韦和达芦那韦)的方案之间的差异。数据来自 MPP 许可方以及大量外部来源。主要结果是在所有 LMIC 中,有和没有 MPP 许可的情况下的成本节约和健康影响。通过其许可,MPP 可以按季度获得在所有涵盖国家/地区销售的许可仿制药的数量和价格。这些数据为过去实际情况下的数量、价格和采用情况提供了信息,并为未来实际情况的建模提供了依据。然后,将这些方案与没有研究许可的一组假设方案进行了比较。
模型的中心假设预测,在 2017 年至 2032 年期间,累积起来,多替拉韦为基础的 HIV 治疗方案的采用量将增加 1549.4 万(范围为 1440.6-1549.4)人年,通过 MPP 许可可以避免 151839 人(34575-312973)死亡,与假设方案相比,节省 30.74 亿美元(18.377-56.177)。对于达芦那韦为基础的 HCV 治疗方案,预计从 2015 年至 2026 年的累积效果将是接受达芦那韦治疗的患者增加 428244 人(127584-636270),避免 4070 人(225-6323)死亡,与假设方案相比,通过许可节省 10.7593 亿美元(30.377-121.284)。
可以对将上游许可与下游结果联系起来的连锁效应进行建模。因此,根据早期仿制药竞争导致价格降低,从而影响采购决策并使推荐药物更快、更广泛地采用的假设,获得了与以获取为导向的自愿许可相关的经济和健康影响的可信定量估计,从而产生了有益的经济和健康影响。
联合国艾滋病规划署。