Department of Research and Development, Netherlands Comprehensive Cancer Organization (IKNL), Utrecht, The Netherlands.
Department of Obstetrics and Gynecology, Radboud Institute for Health Sciences, Radboud University Medical Center, Nijmegen, The Netherlands.
Acta Obstet Gynecol Scand. 2022 Jan;101(1):56-67. doi: 10.1111/aogs.14286. Epub 2021 Nov 1.
Epithelial ovarian cancer (EOC) patients undergoing splenectomy during cytoreductive surgery represent a small subgroup of patients. Splenic metastases or technical reasons due to extensive upper abdominal disease may require a splenectomy. It has been hypothesized that as the spleen's antitumor immunologic functions may inhibit cancer growth, splenectomy may promote the growth of residual disease as observed in other cancer types of murine studies. The few studies assessing the impact of splenectomy on the oncologic outcomes of advanced stage EOC patients have reported inconsistent results. It remains unclear whether splenectomy during cytoreductive surgery is justified to achieve complete cytoreduction. The aim of this study was to assess the impact of a splenectomy on perioperative outcomes and survival of advanced stage EOC patients.
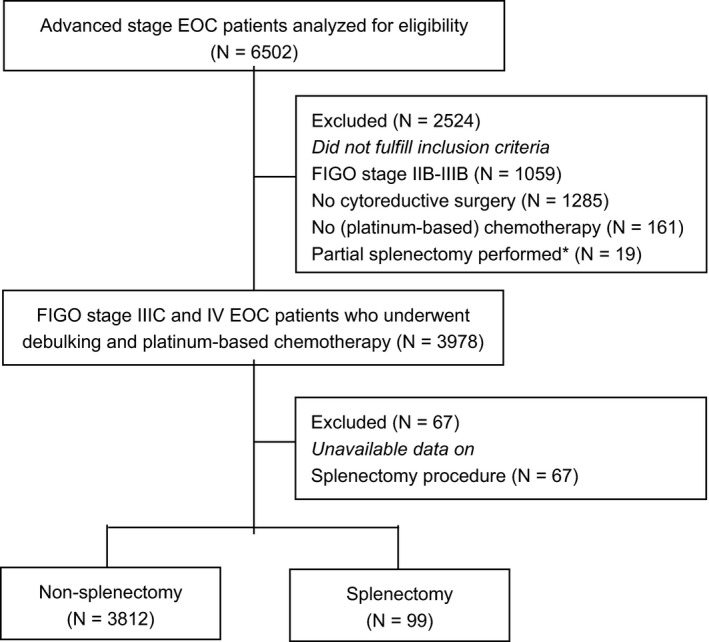
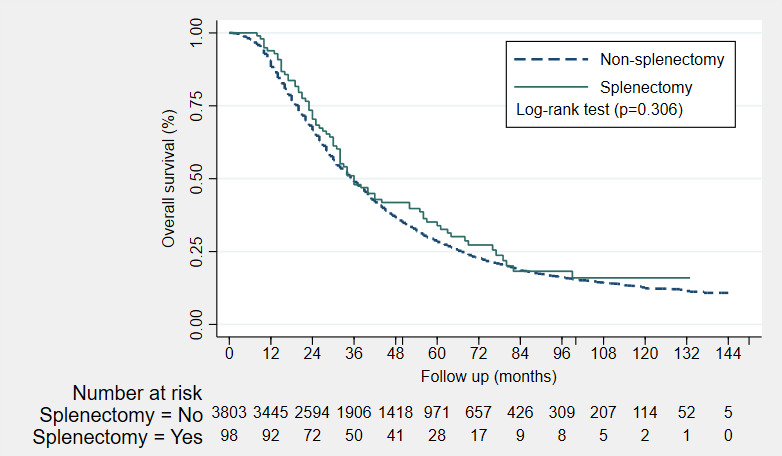
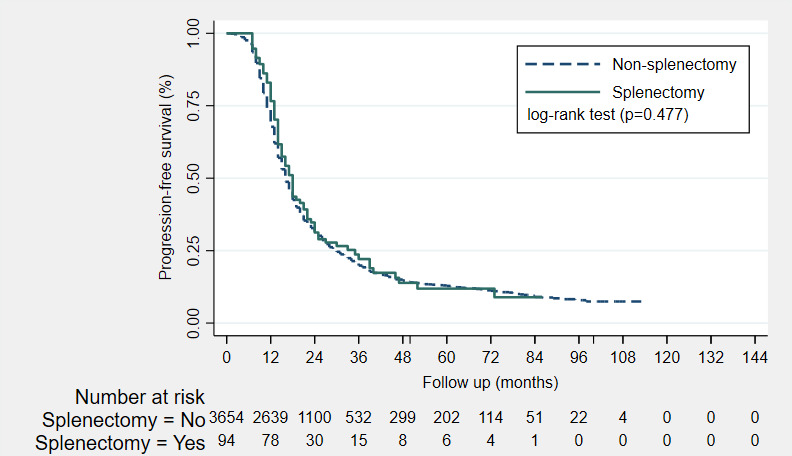
In this nationwide population-based study, all consecutive patients diagnosed with FIGO stage IIIC and IV EOC between 1 January 2008 and 31 December 2015 were identified from the Netherlands Cancer Registry. Patients who underwent cytoreductive surgery combined with platinum-based chemotherapy as primary treatment were selected. Differences in clinicopathologic characteristics between splenectomy and non-splenectomy patients were assessed. Progression-free survival (PFS) and overall survival (OS) were analyzed using Kaplan-Meier survival curves and log-rank tests. Cox proportional hazards models were used to adjust for covariates that influence survival.
A total of 3911 patients were identified: 99 splenectomy and 3812 non-splenectomy patients. Splenectomy patients were more likely to undergo extensive surgery or surgical reintervention, to receive intraperitoneal chemotherapy, intraoperative and postoperative blood transfusion, to experience postoperative infections, and to be admitted to an intensive care unit (all p < 0.002). No significant differences in PFS or OS were observed between splenectomy vs non-splenectomy patients after adjusting for covariates.
Although advanced stage EOC patients who undergo splenectomy during cytoreductive surgery have less favorable perioperative outcomes, no adverse impact of splenectomy on the survival of advanced stage EOC patients was observed. Splenectomy during cytoreductive surgery seems to be justified to achieve complete cytoreduction in advanced stage EOC patients.
在细胞减灭术中接受脾切除术的上皮性卵巢癌(EOC)患者代表了一小部分患者。脾转移或由于广泛的上腹部疾病导致的技术原因可能需要脾切除术。有人假设,由于脾脏的抗肿瘤免疫功能可能抑制癌症生长,因此脾切除术可能会促进残留疾病的生长,正如在其他癌症类型的鼠类研究中观察到的那样。少数评估脾切除术对晚期 EOC 患者肿瘤学结局影响的研究报告了不一致的结果。目前尚不清楚在细胞减灭术中进行脾切除术是否可以达到完全细胞减灭。本研究旨在评估脾切除术对晚期 EOC 患者围手术期结局和生存的影响。
在这项全国性的基于人群的研究中,从荷兰癌症登记处确定了所有在 2008 年 1 月 1 日至 2015 年 12 月 31 日期间诊断为 FIGO 分期 IIIC 和 IV 期 EOC 的连续患者。选择接受细胞减灭术联合铂类化疗作为初始治疗的患者。评估脾切除术和非脾切除术患者之间的临床病理特征差异。使用 Kaplan-Meier 生存曲线和对数秩检验分析无进展生存期(PFS)和总生存期(OS)。使用 Cox 比例风险模型调整影响生存的协变量。
共确定了 3911 名患者:99 名脾切除术患者和 3812 名非脾切除术患者。脾切除术患者更有可能接受广泛手术或手术再干预、接受腹腔内化疗、术中及术后输血、发生术后感染以及入住重症监护病房(均 p<0.002)。调整协变量后,脾切除术与非脾切除术患者的 PFS 或 OS 无显著差异。
尽管在细胞减灭术中接受脾切除术的晚期 EOC 患者的围手术期结局较差,但脾切除术对晚期 EOC 患者的生存没有不利影响。在晚期 EOC 患者中,为达到完全细胞减灭而进行脾切除术似乎是合理的。