North Bay Eye Associates, 104 Lynch Creek Way, Suite 12, Petaluma, CA, 94954, USA.
University of Edinburgh, Edinburgh, UK.
Drugs. 2021 Nov;81(17):2017-2033. doi: 10.1007/s40265-021-01624-9. Epub 2021 Nov 1.
To evaluate the intraocular pressure (IOP)-lowering efficacy and safety of 10 and 15 µg bimatoprost implant in patients with open-angle glaucoma (OAG) or ocular hypertension (OHT).
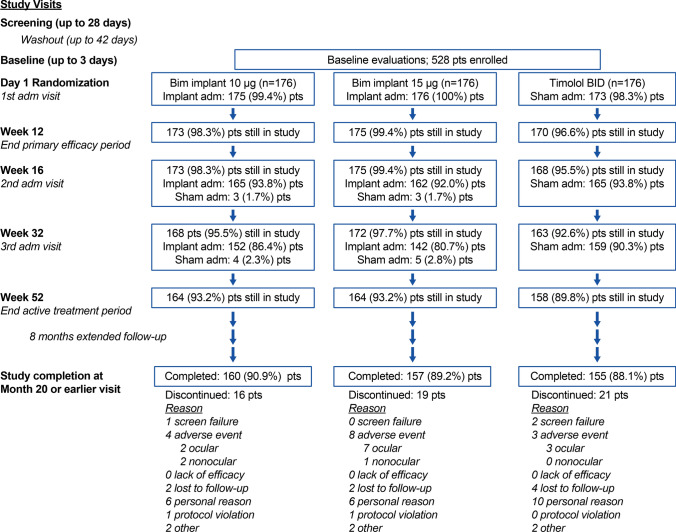
This randomized, 20-month, multicenter, masked, parallel-group, phase 3 trial enrolled 528 patients with OAG or OHT and an open iridocorneal angle inferiorly in the study eye. Study eyes were administered 10 or 15 µg bimatoprost implant on day 1, week 16, and week 32, or twice-daily topical timolol maleate 0.5%. Primary endpoints were IOP and IOP change from baseline through week 12. Safety measures included treatment-emergent adverse events (TEAEs) and corneal endothelial cell density (CECD).
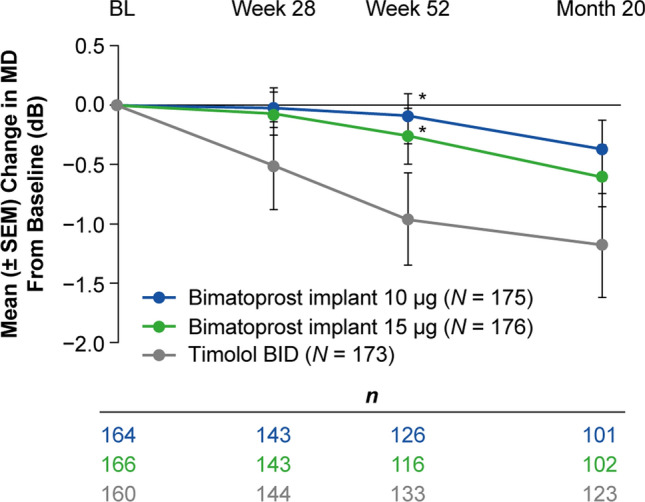
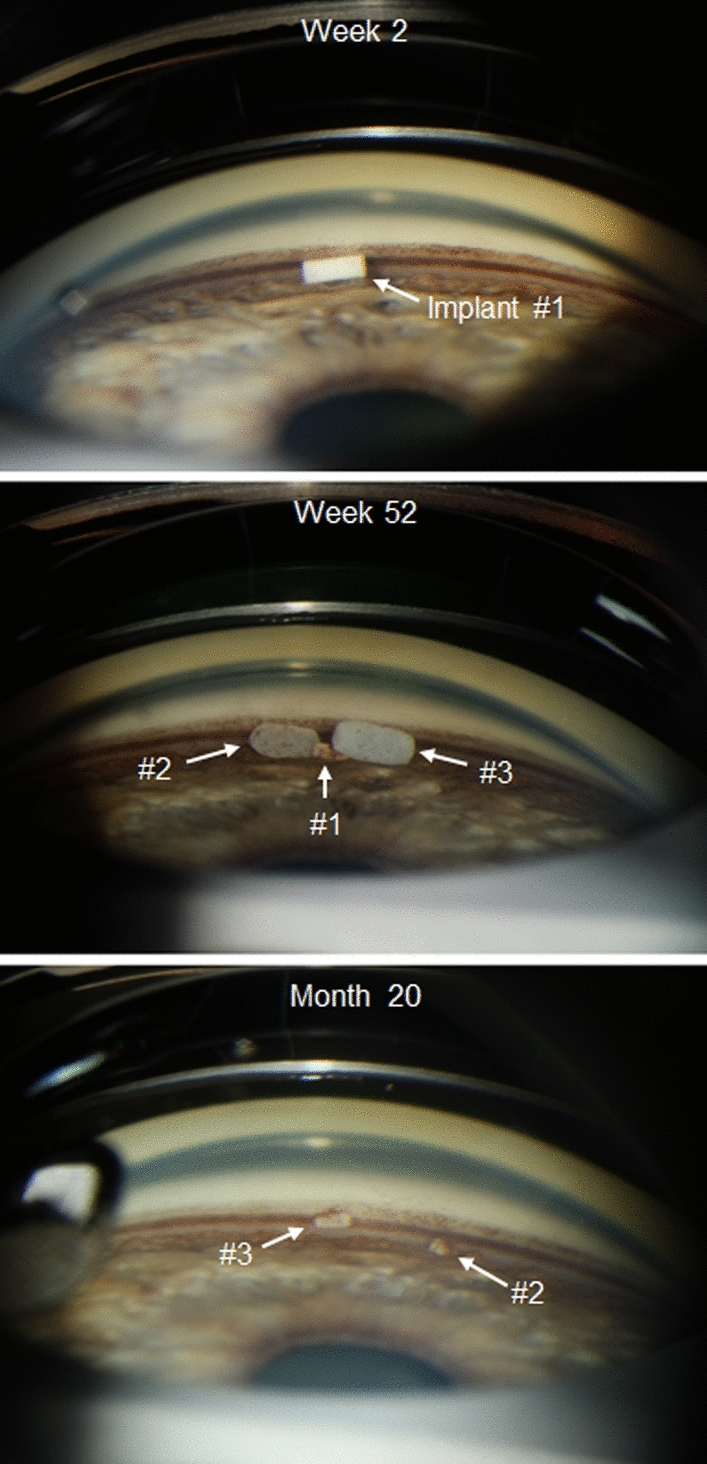
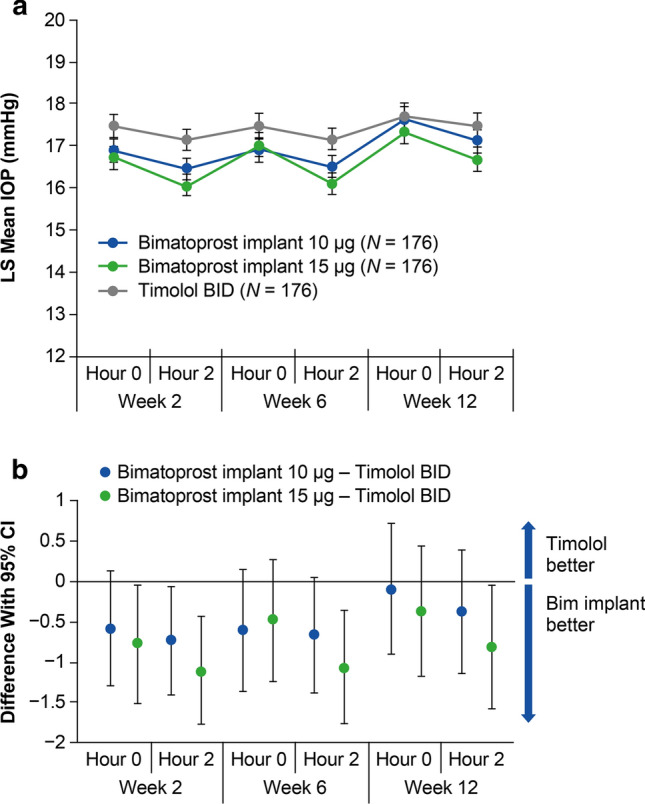
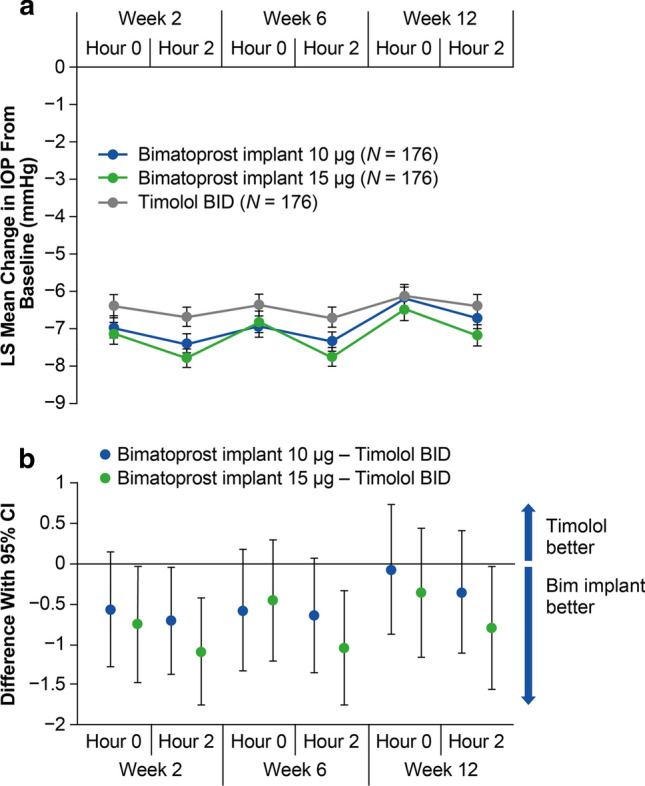
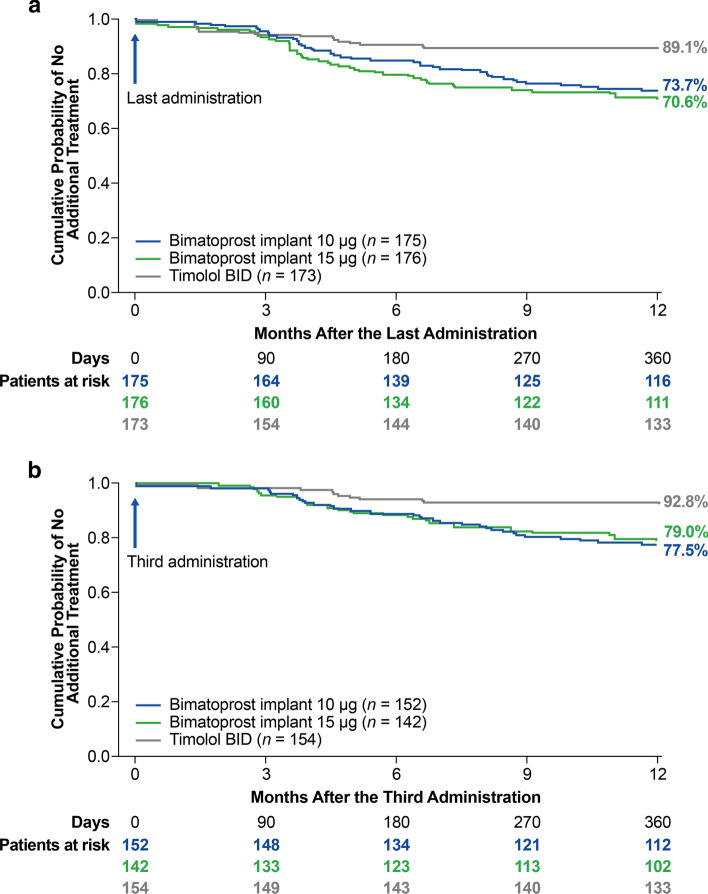
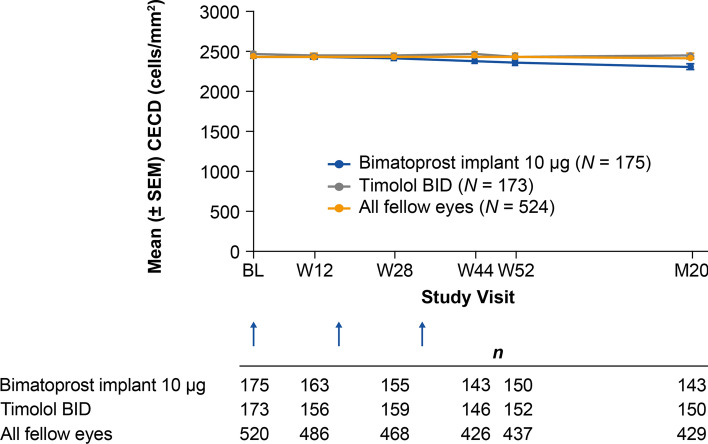
Both 10 and 15 µg bimatoprost implant met the primary endpoint of noninferiority to timolol in IOP lowering through 12 weeks. Mean IOP reductions from baseline ranged from 6.2-7.4, 6.5-7.8, and 6.1-6.7 mmHg through week 12 in the 10 µg implant, 15 µg implant, and timolol groups, respectively. IOP lowering was similar after the second and third implant administrations. Probabilities of requiring no IOP-lowering treatment for 1 year after the third administration were 77.5% (10 µg implant) and 79.0% (15 µg implant). The most common TEAE was conjunctival hyperemia, typically temporally associated with the administration procedure. Corneal TEAEs of interest (primarily corneal endothelial cell loss, corneal edema, and corneal touch) were more frequent with the 15 than the 10 µg implant and generally were reported after repeated administrations. Loss in mean CECD from baseline to month 20 was ~ 5% in 10 µg implant-treated eyes and ~ 1% in topical timolol-treated eyes. Visual field progression (change in the mean deviation from baseline) was reduced in the 10 µg implant group compared with the timolol group.
The results corroborated the previous phase 3 study of the bimatoprost implant. The bimatoprost implant met the primary endpoint and effectively lowered IOP. The majority of patients required no additional treatment for 12 months after the third administration. The benefit-risk assessment favored the 10 over the 15 µg implant. Studies evaluating other administration regimens with reduced risk of corneal events are ongoing. The bimatoprost implant has the potential to improve adherence and reduce treatment burden in glaucoma. CLINICALTRIALS.
NCT02250651.
评估 10 和 15µg 比马前列素植入物在开角型青光眼(OAG)或高眼压症(OHT)患者中的降眼压疗效和安全性。
这是一项随机、20 个月、多中心、盲法、平行组、3 期临床试验,共纳入 528 例 OAG 或 OHT 患者和研究眼中下方开角的虹膜角膜角。研究眼在第 1 天、第 16 周和第 32 周给予 10 或 15µg 比马前列素植入物,或每天两次给予马来酸噻吗洛尔 0.5%。主要终点为第 12 周时的眼压和眼压变化。安全性措施包括治疗中出现的不良事件(TEAEs)和角膜内皮细胞密度(CECD)。
10 和 15µg 比马前列素植入物均符合通过 12 周降低眼压至与噻吗洛尔相当的非劣效性主要终点。第 10µg 植入物、第 15µg 植入物和噻吗洛尔组在第 12 周时的平均眼压降低范围分别为 6.2-7.4mmHg、6.5-7.8mmHg 和 6.1-6.7mmHg。第二次和第三次植入后眼压降低情况相似。第三次给药后 1 年无需降压治疗的概率分别为 77.5%(10µg 植入物)和 79.0%(15µg 植入物)。最常见的治疗相关不良事件是结膜充血,通常与给药过程有关。角膜不良事件(主要为角膜内皮细胞丢失、角膜水肿和角膜触觉)在 15µg 植入物中比 10µg 植入物更常见,通常在多次给药后报告。第 10µg 植入物治疗眼的平均 CECD 从基线到第 20 个月的损失约为 5%,而接受马来酸噻吗洛尔治疗的眼约为 1%。与噻吗洛尔组相比,10µg 植入物组的视野进展(从基线的平均偏差变化)减少。
结果证实了之前关于比马前列素植入物的 3 期研究。比马前列素植入物达到了主要终点,有效降低了眼压。大多数患者在第三次给药后 12 个月内无需额外治疗。与 15µg 植入物相比,10µg 植入物的获益风险评估更有利。正在进行评估其他给药方案的研究,这些方案降低了角膜不良事件的风险。比马前列素植入物有可能改善青光眼患者的依从性并降低治疗负担。临床试验注册号:NCT02250651。