Department of Cardiovascular Medicine, National Cerebral and Cardiovascular Center, 6-1 Kishibe-Shimmachi, Suita, 564-8565, Japan.
Sakakibara Heart Institute of Okayama, Okayama, Japan.
ESC Heart Fail. 2021 Dec;8(6):5617-5621. doi: 10.1002/ehf2.13684. Epub 2021 Nov 2.
The methodology to distinguish between the heart failure (HF) with recovered ejection fraction (HFrecEF) and those with continuously reduced ejection fraction (EF) (HFcrEF) on admission has not been established. We recently demonstrated that the ratio of plasma levels of pro-B-type natriuretic peptide (proBNP) to total BNP (proBNP plus mature BNP) is decreased on admission in patients with mild acute HF, but not in severe acute HF as a compensatory mechanism for activating cyclic GMP via increases of bioactive mature BNP. We aimed to test the hypothesis that the ratio of bioactive mature BNP to total BNP is associated with reverse remodelling capacity in patients with HF with reduced EF.
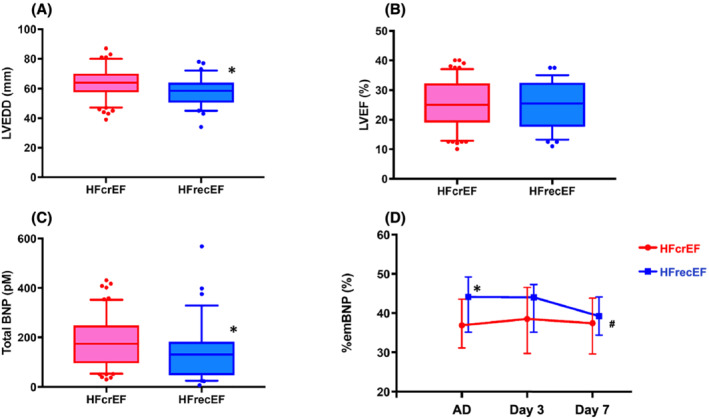
Plasma proBNP and total BNP were measured in patients with acute decompensated HF by using specific and sensitive enzyme immunochemiluminescent assay. Estimated percent mature BNP (%emBNP) was calculated as ([total BNP - proBNP]/total BNP) × 100. We retrospectively identified the patients with reduced EF (≤40%, on admission) who had echocardiographic data after discharge (n = 93). We defined patients with increased EF by >10% during the follow-up term (median, 545 days) after the admission as HFrecEF group. We compared patient characteristics, %emBNP, and other biomarkers between HFrecEF and HFcrEF. Of the enrolled patients with HFrecEF (n = 32) and HFcrEF (n = 61), on admission, %emBNP was significantly higher in HFrecEF than in HFcrEF (44.1% vs. 36.9%; P < 0.05). There were no significant differences in left ventricular EF on admission between the two groups. The univariate analysis revealed that %emBNP on admission was associated with HFrecEF occurrence rate (P < 0.05), in contrast both total BNP and high-sensitive cardiac troponin-T levels were not associated with HFrecEF occurrence rate.
The ratio of mature BNP to total BNP in plasma at the time of hospital admission may be predictive of left ventricular contractile recovery. Preservation of the capacity to convert proBNP to mature BNP, but not myocardial injury itself, is associated with future ventricular contractile recovery.
目前尚无明确方法来区分入院时射血分数恢复的心力衰竭(HFrecEF)和射血分数持续降低的心力衰竭(HFcrEF)。我们最近发现,在轻度急性 HF 患者中,入院时血浆脑钠肽前体(proBNP)与总 BNP(proBNP 加成熟 BNP)的比值降低,但在重度急性 HF 患者中并未降低,这是通过增加生物活性成熟 BNP 激活环鸟苷酸的一种代偿机制。我们旨在验证这样一个假设,即血浆中生物活性成熟 BNP 与总 BNP 的比值与射血分数降低的心力衰竭患者的逆重构能力相关。
采用特定和敏感的酶免疫化学发光测定法检测急性失代偿性心力衰竭患者的血浆 proBNP 和总 BNP。计算估计的成熟 BNP 百分比(%emBNP),计算公式为[总 BNP- proBNP/总 BNP]×100。我们回顾性地确定了入院时射血分数降低(≤40%)且出院后(n=93)有超声心动图数据的患者。我们将随访期间(中位数 545 天)射血分数增加>10%的患者定义为 HFrecEF 组。我们比较了 HFrecEF 和 HFcrEF 患者的临床特征、%emBNP 和其他生物标志物。在纳入的 HFrecEF(n=32)和 HFcrEF(n=61)患者中,HFrecEF 患者的入院时%emBNP 显著高于 HFcrEF(44.1%比 36.9%;P<0.05)。两组入院时左心室射血分数无显著差异。单因素分析显示,入院时%emBNP 与 HFrecEF 发生率相关(P<0.05),而总 BNP 和高敏心肌肌钙蛋白 T 水平与 HFrecEF 发生率无关。
入院时血浆中成熟 BNP 与总 BNP 的比值可能预测左心室收缩功能恢复。保留将 proBNP 转化为成熟 BNP 的能力,而不是心肌损伤本身,与未来心室收缩功能恢复相关。