Valverde-Merino Maria-Isabel, Martinez-Martinez Fernando, Garcia-Mochon Leticia, Benrimoj Shalom I, Malet-Larrea Amaia, Perez-Escamilla Beatriz, Zarzuelo Maria Jose, Torres-Robles Andrea, Gastelurrutia Miguel Angel, Varas-Doval Raquel, Peiro Zorrilla Tamara, Garcia-Cardenas Victoria
Pharmaceutical Care Research Group, University of Granada, Granada, Spain.
Department of Management of Health Services and Professionals, Andalusian School of Public Health, Granada, Spain.
Patient Prefer Adherence. 2021 Oct 24;15:2363-2376. doi: 10.2147/PPA.S330371. eCollection 2021.
It is necessary to determine the cost utility of adherence interventions in chronic diseases due to humanistic and economic burden of non-adherence.
To evaluate, alongside a cluster-randomized controlled trial, the cost-utility of a pharmacist-led medication adherence management service (MAMS) compared with usual care in community pharmacies.
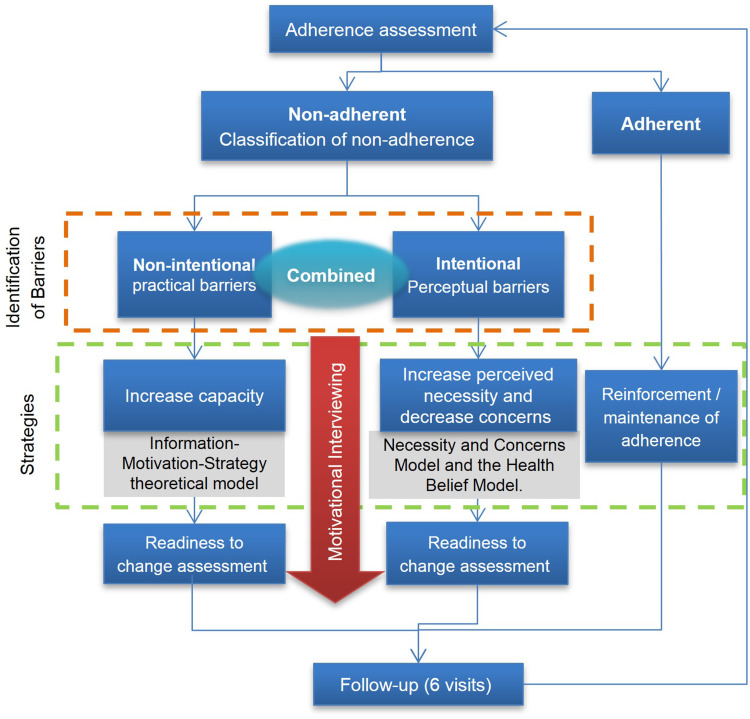
The trial was conducted over six months. Patients with treatments for hypertension, asthma or chronic obstructive pulmonary disease (COPD) were included. Patients in the intervention group (IG) received a MAMS based on a brief complex intervention, whilst patients in the control group (CG) received usual care. The cost-utility analysis adopted a health system perspective. Costs related to medications, healthcare resources and adherence intervention were included. The effectiveness was estimated as quality-adjusted life years (QALYs), using a multiple imputation missing data model. The incremental cost-utility ratio (ICUR) was calculated on the total sample of patients.
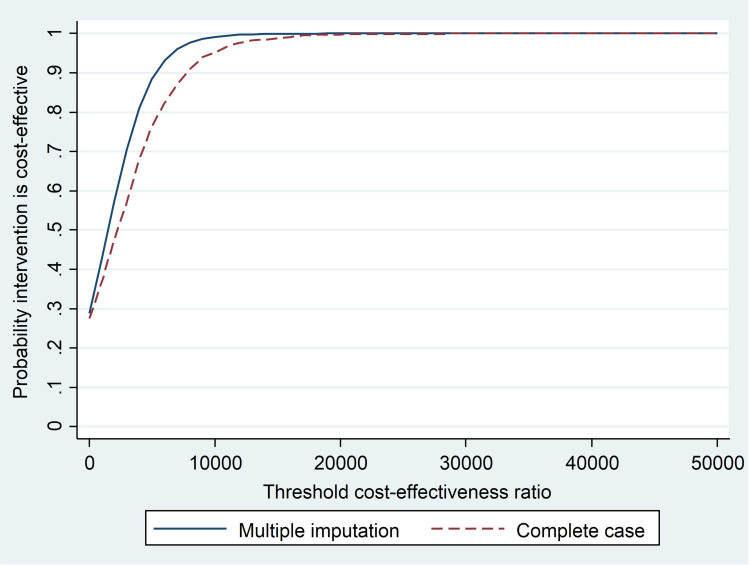
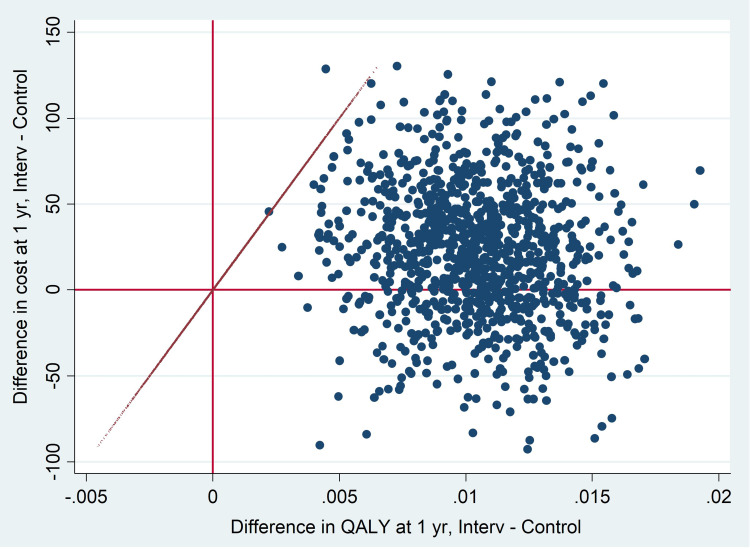
A total of 1186 patients were enrolled (IG: 633; CG: 553). The total intervention cost was estimated to be €27.33 ± 0.43 per patient for six months. There was no statistically significant difference in total cost of medications and healthcare resources per patient between IG and CG. The values of EQ-5D-5L at 6 months were significantly higher in the IG [IG: 0.881 ± 0.005 vs CG: 0.833 ± 0.006; p = 0.000]. In the base case, the service was more expensive and more effective than usual care, resulting in an ICUR of €1,494.82/QALY. In the complete case, the service resulted in an ICUR of €2,086.30/QALY, positioned between the north-east and south-east quadrants of the cost-utility plane. Using a threshold value of €20,000/QALY gained, there is a 99% probability that the intervention is cost-effective.
The medication adherence management service resulted in an improvement in the quality of life of the population with chronic disease, with similar costs compared to usual care. The service is cost-effective.
由于不依从带来的人文和经济负担,有必要确定慢性病依从性干预措施的成本效益。
在一项整群随机对照试验的同时,评估由药剂师主导的药物依从性管理服务(MAMS)与社区药房常规护理相比的成本效益。
试验持续六个月。纳入接受高血压、哮喘或慢性阻塞性肺疾病(COPD)治疗的患者。干预组(IG)患者接受基于简短综合干预的MAMS,而对照组(CG)患者接受常规护理。成本效益分析采用卫生系统视角。纳入了与药物、医疗资源和依从性干预相关的成本。使用多重填补缺失数据模型将有效性估计为质量调整生命年(QALY)。对患者总样本计算增量成本效益比(ICUR)。
共纳入1186例患者(IG:633例;CG:553例)。六个月期间每位患者的总干预成本估计为27.33±0.43欧元。IG组和CG组每位患者的药物和医疗资源总成本无统计学显著差异。IG组在6个月时的EQ-5D-5L值显著更高[IG:0.881±0.005 vs CG:0.833±0.006;p = 0.000]。在基础案例中,该服务比常规护理更昂贵且更有效,ICUR为1494.82欧元/QALY。在完整案例中,该服务的ICUR为2086.30欧元/QALY,位于成本效益平面的东北和东南象限之间。使用每获得一个QALY 20000欧元的阈值,该干预措施具有成本效益的概率为99%。
药物依从性管理服务改善了慢性病患者的生活质量,与常规护理相比成本相似。该服务具有成本效益。