Department of Neurology, Bangur Institute of Neurosciences, IPGMER and SSKM Hospital, Annex 1, 52/1 Shambhunath Pandit Street, Kolkata, 700020, India.
Department of Internal Medicine, RG Kar Medical College and Hospital, 1, Khudiram Bose Sarani, Kolkata, 700004, India.
Diabetes Metab Syndr. 2021 Nov-Dec;15(6):102326. doi: 10.1016/j.dsx.2021.102326. Epub 2021 Oct 29.
The COVID-19 pandemic has turned the world topsy turvy since its emergence and has claimed innumerable lives worldwide. Neurological manifestations of the disease have raised several eyebrows around the world among which Guillain-Barré syndrome (GBS) deserve special mention. Although majority of the cases of the coronavirus disease 2019 (COVID-19) present with respiratory symptoms, extrapulmonary manifestations are being increasingly reported. We conducted this study to analyze detailed clinical presentations and outcome in a series of eight cases (n = 8) with COVID-19 associated GBS.
An observational prospective study was conducted among patients with post-infectious/para-infectious GBS. 8 patients were subclassified into acute inflammatory demyelinating polyneuropathy (AIDP), acute motor axonal neuropathy (AMAN) and acute motor and sensory axonal neuropathy (AMSAN) as per electrodiagnostic criteria and were followed up from admission to 6 months post discharge, to obtain a comprehensive clinical profile and outcome in these patients.
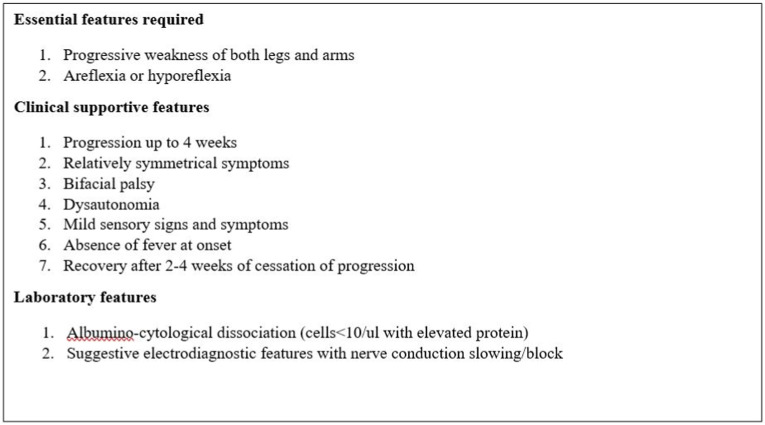
The diagnosis of GBS was confirmed as per Asbury criteria, supported by electrodiagnostic features in nerve conduction velocity test. Among the series of 8 patients, 3 were diagnosed as AIDP, 3 had AMAN and the remaining 2 patients had AMSAN. 3 patients of GBS were afebrile and were diagnosed as COVID-19 after a positive assay on routine screening. Cerebro-spinal fluid analysis for SARS-Cov-2 RT-PCR and serum anti-ganglioside antibodies were negative in all the patients.
GBS in patients with COVID-19 should be differentiated from critical illness neuropathy and myopathy. Early diagnosis is important as it is associated with poor outcome and prolonged invasive ventilation.
自 COVID-19 出现以来,它使世界变得混乱不堪,并在全球范围内夺走了无数人的生命。该疾病的神经系统表现引起了全球的关注,其中吉兰-巴雷综合征(GBS)值得特别提及。尽管大多数 COVID-19 病例表现出呼吸道症状,但越来越多的报道表明存在肺外表现。我们进行这项研究是为了分析 8 例 COVID-19 相关 GBS 患者的详细临床表现和结局。
对感染后/感染性疾病相关 GBS 患者进行观察性前瞻性研究。根据电诊断标准,8 例患者被分为急性炎症性脱髓鞘性多发性神经病(AIDP)、急性运动轴索性神经病(AMAN)和急性运动感觉轴索性神经病(AMSAN),并从入院到出院后 6 个月进行随访,以获得这些患者的综合临床特征和结局。
根据 Asbury 标准并结合神经传导速度测试中的电诊断特征,确诊为 GBS。在这 8 例患者中,3 例诊断为 AIDP,3 例诊断为 AMAN,其余 2 例诊断为 AMSAN。3 例 GBS 患者无发热,在常规筛查中检测到阳性后被诊断为 COVID-19。所有患者的脑脊液分析均未检出 SARS-CoV-2 RT-PCR 和血清抗神经节苷脂抗体。
COVID-19 患者的 GBS 应与危重病性神经病和肌病相区别。早期诊断很重要,因为它与不良结局和延长的有创通气有关。